Arthroscopic Reduction and Fixation of Distal Radius and Ulnar Styloid Fractures
DEFINITION
A bimodal age distribution exists for patients with distal radius fractures (ie, young adults vs. elderly persons), and they frequently have a different mechanism of injury.Patients 65 years of age or older have an annual incidence of 8 to 10 fractures of the distal radius per 1000 person-years.The incidence is seven times higher in women than in men.Sixteen percent of white women and 23% of white men will sustain a fracture of the distal radius after the age of 50 years.Fractures of the distal radius are one of the most common skeletal injuries treated by orthopaedic surgeons.These injuries account for one-sixth of all fractures that are evaluated in the emergency department. Displaced intra-articular fractures of the distal radius are a unique subset of radius fractures. 25These fractures are a high-energy injury.This high-energy injury results in comminuted fracture patterns.These fractures are less amenable to traditional closed manipulation and casting.The prognosis for these fractures depends on the amount of residual radius shortening, both radiocarpal and radioulnar articular congruity, and associated soft tissue injuries. 31
ANATOMY
The distal radius serves as a plateau to support the carpus.The distal radius has three concave articular surfaces: the scaphoid fossa, the lunate fossa, and the sigmoid notch.The distal articular surface of the radius has a radial inclination averaging 22 degrees and palmar tilt averaging 11 degrees.Radial-based volar and dorsal ligaments arise from the distal radius to support the wrist. The sigmoid notch of the distal radius articulates with the ulnar head about which it rotates.The distal radioulnar joint (DRUJ) is primarily stabilized by the triangular fibrocartilage complex (TFCC).The sigmoid notch angles distally and medially at an average of 22 degrees.
PATHOGENESIS
The biomechanical characteristics of each fracture type depend on the mechanism of injury.Fernandez and Geissler 11 developed a classification based on the mechanism of injury. They noted that the associated ligamentous lesions, subluxations, and associated carpal fractures are related directly to the degree of energy absorbed by the distal radius.Type I fractures are bending fractures of the metaphysis in which one cortex fails due to tensile stress and the opposite one undergoes a certain degree of comminution (eg, extra-articular Smith or Colles fractures).Type II fractures are shearing fractures of the joint surface (eg, radial styloid fractures, Barton fracture).Type III fractures are compression fractures of the joint surface with impaction of the subchondral and metaphyseal cancellous bone (ie, intra-articular comminuted fractures).Type IV fractures are avulsion fractures of ligamentous attachments, including radial styloid and ulnar styloid fractures, and are associated with radiocarpal fracture-dislocations.Type V fractures are high-energy injuries that involve a combination of bending, compression, shearing, and avulsion mechanisms or bone loss.Several studies have shown that a high incidence of associated soft tissue injuries is seen with displaced intraarticular distal radius fractures. 16,18,19,20,24,26,29Arthroscopic studies demonstrate a high incidence of injury to the TFCC, followed by the scapholunate interosseous ligament (SLIL), and then the lunotriquetral interosseous ligament (LTIL) (which is the least injured).A spectrum of injury occurs to the interosseous ligament in which it attenuates and eventually tears and the degree of rotation between the carpal bones increases.Geissler et al 15 defined an arthroscopic classification of interosseous ligament tears that helps define the degree of ligament injury and secondary instability as well as proposes treatment (Table 1; see also Chap. 67).
NATURAL HISTORY
Intra-articular fractures of the distal radius have two pathologies: the associated global injury to the soft tissues and the injury to the bone itself.The natural history for an intra-articular fracture of the distal radius depends on restoration of anatomy as well as detection and management of any associated soft tissue injuries. 4,11Knirk and Jupiter 20 documented the importance of articular restoration over extra-articular orientation in predicting outcomes for fractures of the distal radius.They showed solid evidence that the largest tolerable articular step-off is 2 mm.They demonstrate that the better the restoration of the articular surface, the better the outcome.A loss in radius length of 2.5 mm will shift the normal load transmitted across the ulna from 20% to 42%, which may lead to various stages of ulnar impaction syndrome.SLIL and TFCC injuries are often associated with distal radius fractures and may be missed on plain x-ray.In one study, nearly one-third of fractures had an associated SLIL injury and greater than 60% had a TFCC injury. 1P.263 Table 1 Geissler Arthroscopic Classification of Carpal Instability Grade|
DEFINITION
|Arthroscopic Findings|Management------|---1.Attenuation/hemorrhage of interosseous ligament as seen from the radiocarpal joint. No incongruency of carpal alignment in the midcarpal space.There is a loss of the normal concave appearance between the carpal bones, and the interosseous ligament attenuates and becomes convex as seen from the radiocarpal space. In midcarpal space, the interval between the carpal bones will still be tight and congruent, with no step-off.Immobilization2.Attenuation/hemorrhage of the interosseous ligament as seen from the radiocarpal joint. Incongruency/step-off as seen from the midcarpal space. A slight gap between the carpal bones may be present.A slight gap (less than the width of a probe) between the carpal bones may be present. The interosseous ligament continues to become attenuated and is convex as seen from the radial carpal space. In the midcarpal space, the interval between the involved carpal bones is no longer congruent, and a step-off is present. In scapholunate instability, palmar flexion of the dorsal lip of the scaphoid will be seen as compared to the lunate. In lunotriquetral instability, increased translation between the triquetrum and lunate will be seen when palpated with a probe.Arthroscopic reduction and pinning3.Incongruency/step-off of carpal alignment is seen in both the radiocarpal and midcarpal spaces.The interosseous ligament has started to tear, usually from volar to dorsal, and a gap is seen between the carpal bones in the radiocarpal space. A probe often is helpful to separate the involved carpal bones in the radiocarpal space. In the midcarpal space, a 2-mm probe may be placed between the carpal bones and twisted.Arthroscopic/open reduction and pinning4.Incongruency/step-off of carpal alignment is seen in both the radiocarpal and midcarpal spaces. Gross instability with manipulation is noted.A 2.7-mm arthroscope may be passed through the gap between the carpal bones. The interosseous ligament is completely detached between the involved carpal bones. This is the “drive-through” sign, when the arthroscope may be freely passed from the radiocarpal space through the tear to the midcarpal space.Open reduction and repairIn another study, SLIL injuries were found in more than half, LTIL injuries in one-third, and TFCC in 60%. Only 17% of patients were free of any of the three injuries. 28Untreated complete tears of the SLIL, which are highly associated with radial styloid fractures, may progress to a wrist with scapholunate advanced collapse.
PATIENT HISTORY AND PHYSICAL FINDINGS
A thorough history should be obtained, including the circumstances surrounding the injury as well as any additional injuries.Neurologic basis Cardiac basisPatients' level of independence, dominant hand, status with assisted devices, work, activity level, and support structure should be determined.Physical examination, while concentrating on the wrist, should also include the hand, elbow, and shoulder to check for concomitant injuries.The hand, wrist, forearm, arm, and shoulder must be carefully inspected for open injury so that tetanus and antibiotic prophylaxis may be initiated if necessary.A thorough distal sensory and motor function examination should be carried out in an organized manner.Vascular examination should include palpation of both the radial and ulnar pulses and determination of capillary refill time.Precise palpation is used to define areas of potential trauma.Diminished sensibility, pallor, altered capillary refill, increased tenseness of the soft tissues, and pain out of proportion should raise suspicion for significant soft tissue injury, including compartment syndrome.
IMAGING AND OTHER DIAGNOSTIC STUDIES

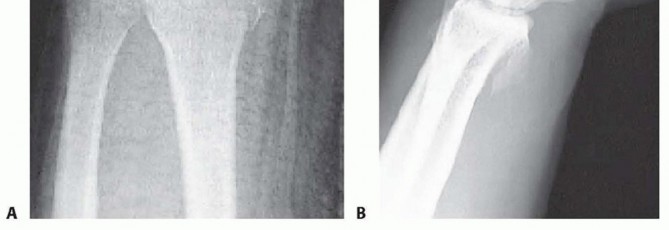
FIG 1 • A. PA radiographic view showing a minimally displaced radial styloid fracture fragment. B. The lateral view shows a complete fracture-dislocation of the wrist. A modified lateral radiograph with the beam angulating 10 to 30 degrees proximally improves visualization of the articular surface and evaluation of the volar rim of the lunate facet represented by the anterior teardrop.An additional 30-degree anteroposterior (AP) cephalic projection is useful to evaluate the dorsal ulnar margin of the distal radius.Oblique radiographs are very helpful because major fracture fragments may be rotated out of their anatomic planes.Computed tomography (CT) evaluation, particularly three-dimensional CT, can further delineate fragment location, joint compression, and rotation.Magnetic resonance imaging (MRI) evaluation is useful in assessing for associated soft tissue injuries such as TFCC tears, interosseous ligament injuries, and carpal fractures.Radiographic signs that demonstrate that the distal radius fracture is likely unstable and closed reduction would be insufficient include the following 21:Lateral tilt greater than 20 degrees dorsalDorsal comminution greater than 50% of the lateral width Initial fragment displacement greater than 1 cmVolar translation greater than 2 mm Initial radius shortening more than 5 mm Intra-articular step-off greater than 2 mm Associated ulnar fractureSevere osteoporosis Age older than 60 years
DIFFERENTIAL DIAGNOSIS
Carpal bone fractureMetacarpal or phalangeal fracture DRUJ disruptionEssex-Lopresti lesion Interosseous ligament tear Carpal dislocation (perilunate)
NONOPERATIVE MANAGEMENT
Displaced fractures of the distal radius are reduced using an adequate anesthetic agent.Knowledge of the mechanisms of injury helps facilitate manual reduction. Force is applied opposite the force that caused the fracture.Gentle traction is necessary to disimpact the fracture fragments, followed by palmar translation of the hand and carpus in respect to the radius.The radius articular surface will rotate around the intact volar cortical lip to restore volar inclination with palmar translation.Care must be taken to avoid trauma to the skin during the reduction maneuver, particularly in elderly patients where the skin may be fragile.A splint is supplied following the reduction. No consensus has been established regarding wrist or forearm position, long-arm versus short-arm immobilization, or splint versus cast.Extreme positions of wrist flexion and ulnar deviation should be avoided. Postreduction radiographs are taken in plaster.Depending on stability of the fracture, most patients treated nonoperatively require weekly visits for the first 3 weeks to monitor fracture reduction.In patients older than 65 years, one-third of initially undisplaced fractures subsequently collapsed to some degree.One study of elderly patients with moderately displaced fractures of the distal radius found that two-thirds of the correction obtained by closed manipulation was lost at 5 weeks.Patients with minimally displaced or nondisplaced fractures of the distal radius treated nonoperatively must be made aware of possible complications, including rupture of the extensor pollicis longus tendon, carpal tunnel syndrome, and compartment syndrome.Elderly patients typically tolerate nonoperative management well.Patients older than 65 years undergoing nonoperative results have comparable results to those that undergo operative treatment despite unsatisfactory radiographic outcomes. 2,3
SURGICAL MANAGEMENT
Distal radius fractures without extensive metaphyseal comminution are ideal candidates for arthroscopic-assisted fixation with K-wires or cannulated screws. 14,15,22Radial styloid fractures Impacted fracturesDie-punch fracturesThree-part T-type fractures and four-part fractures with metaphyseal comminution are best treated with a combination of volar plate stabilization. Wrist arthroscopy is used as an adjunct to fine-tune the articular reduction and evaluate for associated soft tissue lesions.Distal radius fractures that may be minimally displaced, and fractures with strongly suspected associated soft tissue injury, also are candidates for arthroscopic-assisted fixation to stabilize the fracture but, more importantly, to evaluate and treat the acute associated soft tissue injury.Stabilization of associated ulnar styloid fragments is controversial. 20 Wrist arthroscopy provides a rationale as to when to stabilize an ulnar styloid fragment.
PREOPERATIVE PLANNING
All radiographic studies are reviewed.Equipment needed for arthroscopic treatment and for open stabilization is made available.Small joint instrumentation is essential for arthroscopic-assisted fixation of distal radius fractures. The small jointP.265arthroscope is approximately 2.7 mm in diameter, and even smaller scopes may be used if desired. In addition, a small joint shaver (3.5 mm or less) is useful to clear fracture debris and hematoma.The ideal timing for arthroscopic-assisted fixation of distal radius fractures is 3 to 10 days following injury. 13Earlier attempts at fixation may be complicated by soft tissue swelling and troublesome bleeding, obscuring visualization.After 10 days, the fracture fragments start to become sticky and more difficult to percutaneously elevate and reduce.
POSITIONING
Arthroscopic-assisted fixation of distal radius fractures may be performed with the arm suspended vertically in a traction tower, horizontally in a traction tower, or with finger traps applied attached to weights hanging over the edge of the hand table.Wrist arthroscopy in the horizontal position may make it easier to simultaneously monitor the reduction fluoroscopically and place hardware. However, it does not allow for simultaneous volar access to the wrist.Suspending the wrist in a vertical position with a traction tower allows simultaneous access to both the volar and dorsal aspects of the wrist. This is particularly useful when wrist arthroscopy is used as an adjunct to volar plate fixation of the distal radius fracture.A new traction tower has been designed to allow simultaneous evaluation of the intra-articular reduction of the distal radius arthroscopically and fluoroscopically ( FIG 2A).The surgeon may stabilize a comminuted fracture of the distal radius with a plate, and simultaneously evaluate the articular reduction arthroscopically.The traction tower allows for traction of the wrist in either the vertical or horizontal planes, depending on the surgeon's preference ( FIG 2B).
APPROACH




FIG 2 • A. This traction tower uses a suspension bar at the side rather than at the center of the wrist. This allows easy fluoroscopic evaluation of the fracture reduction, with simultaneous full access to the volar and dorsal aspects of the wrist. B. The tower can be flexed into a horizontal position for surgeons who prefer to treat distal radius fractures in that position. It is difficult to palpate the normal extensor tendon landmarks for traditional wrist arthroscopy in patients whosustain a fracture of the distal radius because of swelling. 17 However, the bony landmarks usually can still be palpated. These bony landmarks include the bases of the metacarpals, the dorsal lip of the radius, and the ulnar head.The 3-4 portal is made in line with the radial border of the long finger. It is very useful to place an 18-gauge needle into the proposed location of the 3-4 portal before making a skin incision.If the portal is placed too proximal, the arthroscope may be placed within the fracture pattern itself. If it is placed too distal, it can injure the articular surface of the carpus.Once the precise ideal location of the portal is located, the portal is made by pulling the skin with the surgeon's thumb against the tip of a no. 11 blade. Blunt dissection is carried down with a hemostat, and the arthroscope, with a blunt trocar, is introduced into the dorsal 3-4 portal.This technique decreases potential injury to cutaneous nerves.Thorough irrigation of the joint is necessary to wash out fracture hematoma and debris and improve visualization. Inflow may be provided through the arthroscope cannula or separately through a 14-gauge needle into the 6U portal.Use of a separate 6U inflow portal is recommended. The small joint arthroscopy cannula does not allow as much space between the cannula and the arthroscope, limiting the amount of flow through the cannula.Outflow to the wrist is provided through intravenous extension tubing connected to the arthroscope cannula.The 4-5 working portal is made in line with the mid-axis of the ring metacarpal. Alternatively, the 6R working portal is made just radial to the palpable extensor carpi ulnaris tendon.An 18-gauge needle is placed into the joint and should lie just distal to the articular disc.A 4-5 or 6R portal usually is located just proximal to the 3-4 portal because of the natural radial slope of the distal radius.P.266More recently, del Piñal et al 7 described a dry arthroscopy technique in order to avoid the risk of compartment syndrome from fluid infusion.Although the setup is similar, there have been a few notable difficulties that are associated with the lack of fluid infusion.To avoid fogging of the arthroscope, the scope should be warmed in warm saline prior to placing it in the wrist or by adding anti-fog drops to the end of the scope.The arthroscope valve is left in the open position to prevent collapse of the capsule, and a shaver is placed in the 6R portal on suction to help clear debris and blood.Hematoma and debris will still need to be occasionally flushed through the joint with saline for adequate visualization.
TECHNIQUES
RADIAL STYLOID FRACTURES
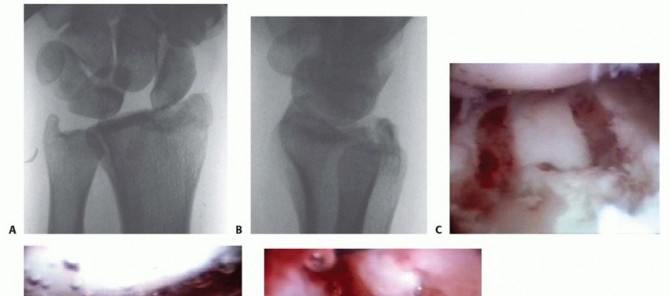
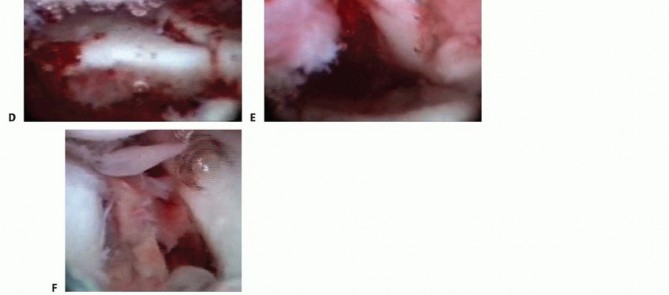
TECH FIG 2 • A. PA view showing an impacted scaphoid facet fracture fragment with an obvious injury to the SLIL. B. Lateral view showing a dorsal rim fracture fragment. C. The arthroscope is in the 6R portal, demonstrating the impacted scaphoid facet fracture fragment. This would be quite difficult to view through an open arthrotomy but is well visualized arthroscopically under bright light and magnified conditions. D.
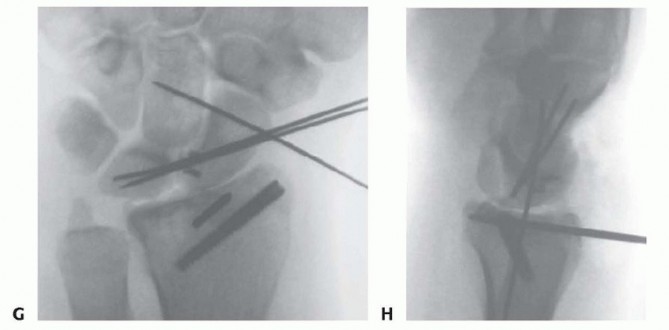
TECH FIG 2 •(continued)G,H. PA and lateral radiographs showing anatomic reduction to the impacted scaphoid facet fracture. (The tear of the SLIL also was acutely repaired.)

TECH FIG 3 • A. The PA radiograph shows a displaced fracture of the radial styloid. B. This lateral radiograph shows metaphyseal comminution associated with the displaced radial styloid fragment. Because of the metaphyseal comminution, it was decided to stabilize the fracture using a volar plate.
OPEN REDUCTION AND STABILIZATION
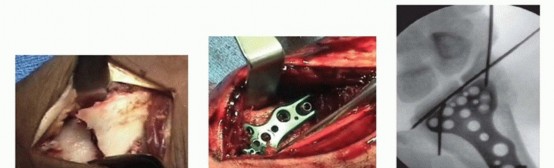
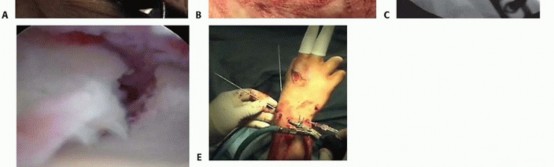


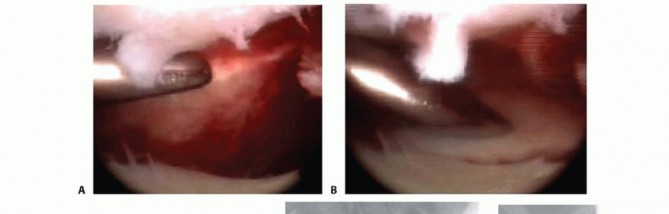
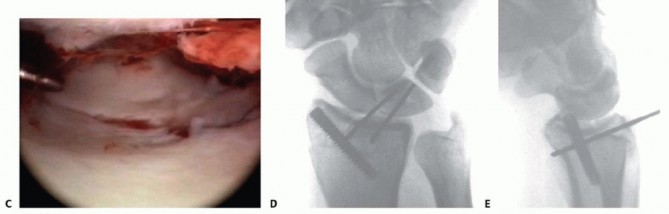
TECH FIG 4 • A. A standard volar approach is made, centered over the flexor carpi radialis tendon, and the fracture site is exposed. B. A volar distal radius locking plate is applied. The initial screw is placed through the proximal plate to secure the plate to the shaft. C. The intra-articular reduction is viewed under fluoroscopy and provisionally pinned. A displaced intra-articular fracture fragment can still be identified. D. The arthroscope is in the 3-4 portal, showing the volar capsule blocking reduction of the radial styloid fragment. E. Joysticks previously inserted into the radial styloid fragment are then used to control and anatomically reduce the radial styloid fragment. F. The arthroscope is in the 6R portal looking across the wrist. Anatomic reduction of the radial styloid fragment is documented. G. Once the anatomic restoration of the articular surface is evaluated both arthroscopically and fluoroscopically, the distal screws are placed in the plate. H. Fluoroscopic view showing anatomic restoration to the articular surface of the distal radius. I. The patient had an associated osteochondral fracture of the lunate, not visible on plain radiographs. The displaced fragment is arthroscopically removed. P.270Apply a volar distal radius locking plate to stabilize the volar bone fragments ( TECH FIG 4B).Place a screw in the proximal portion of the plate first to reduce the plate to the shaft.Provisionally pin the distal fragments through the plate.Manipulate the articular fragments under fluoroscopy to obtain as anatomic a reduction as possible ( TECH FIG 4C,D).Suspend the wrist in the traction tower and reduce the articular fragments arthroscopically ( TECH FIG 4E,F).If articular reduction is not anatomic, remove the pins and fine-tune the reduction.Once the fracture reduction is thought to be anatomic, place the distal screws through the plate ( TECH FIG 4G-I).It is important that the fracture be reduced to the plate, with no gap between the plate and the bone. This can be achieved by flexion of the wrist in the tower and by insertion of a nonlocking screw first, before the insertion of standard locking screws.Place the remaining proximal and distal screws if the reduction is anatomic under both fluoroscopy and arthroscopy. Reduction and Stabilization of a Dorsal Die-Punch Fragment
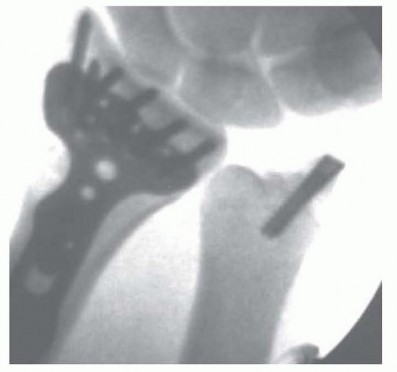
TECH FIG 5 • In this case, following reduction to the distal radius fracture, the articular disc was palpated and found to be lax but with no peripheral tear. The large ulnar styloid fragment was reduced with a micro Acutrak screw.
Intra-articular Distal Radius Fracture Malunion
Malunion of a distal radius fracture can rapidly lead to a degenerative joint in active individuals.
Immediate correction of the malunion is needed for any chance of stopping degeneration of the articular surface.
Correction of the malunion under arthroscopy allows both the ability to access the current state of the joint surface and assures adequate alignment of the fractures while providing good long-term results. Recently,
this is has been described by del Piñal et al. 5,6
The hand is placed into traction, and standard 3-4 and 6R portals are developed as previously described.
P.271
Place the arthroscope into the 3-4 portal to visualize the joint surface.
If severe chondral defects are noted, then either an arthroplasty or arthrodesis should be considered.
The joint will often be filled with synovitis and fibrin debris. A shaver is placed into the 6R position, and the joint is cleared of the debris to obtain adequate visualization.
The hand is removed from traction and a volar plate is placed as previously described through a volar approach and attached to the shaft.
Next place the hand back into traction and place the arthroscope back into the 6R portal to visualize the malunited fragments. A volar radial portal may be placed at this time to be used for instruments along with the 3-4 portal.
Osteotomes are then introduced for cutting the fragments through the 3-4 and volar radial portal by introducing the blade parallel to the tendons and then rotating it into the joint.
The osteotomes are then advanced over the external callus to free up the individual fragments.
Care should be taken to not overshoot the joint and plunge the osteotome volarly or dorsally potentially severing tendons.
The fragments are then elevated either with a probe or percutaneously.
After the fragments have been elevated, the locking pegs of the plate are then advanced as previously described.
INTRA-ARTICULAR DISTAL RADIUS FRACTURE MALUNION
ARTHROSCOPIC RESECTION ARTHROPLASTY
Patients with severe loss of cartilage of the carpus should be considered for salvage procedures such as total wrist arthrodesis or arthroplasty.Although results are early, del Piñal et al 8 demonstrated that good pain relief and return of motion could be obtained by resecting the fragments and creating a smoother joint surface. This could provide a temporarytreatment for active patients and possibly a definitive treatment for low-demand patients. 8Diagnostic arthroscopy is first performed. Evaluation of the midcarpus must be performed to exclude pathology at this site.Typically, there is significant amount of debris and synovitis that must be débrided with a shaver to visualize the radiocarpal joint.A burr is then placed in the radiocarpal joint to smooth the raised malunited cancellous surface of the radius to a level slightly below the normal cartilaginous surface.The injured area of carpus is then likewise débrided with a shaver to obtain a smooth surface.Patients are started on range-of-motion exercises immediately unless excluded by other concomitant procedures.PEARLS AND PITFALLS
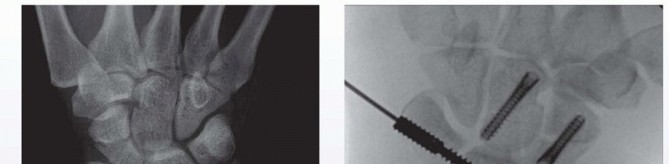
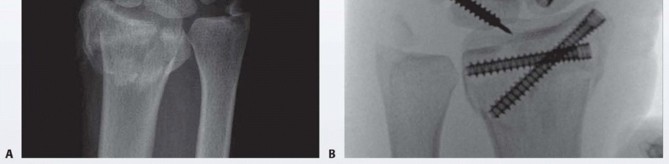
FIG 3 • A. AP radiographic view showing three-part intra-articular distal radius fracture along with an obvious transverse scaphoid fracture. A more subtle capitate fracture is also seen. B. An intraoperative PA radiographic view is seen. The patient required two Acutrack (Acumed, Hillsboro, OR) cannulated compression screws for repair of the distal radius fracture. The capitate and scaphoid were likewise repaired using Acutrack cannulated screws. Intraoperatively, a lunotriquetral ligament tear was seen and the interval stabilized with an Acumed Scapholunate Intercarpal (SLIC) screw (Acumed).
POSTOPERATIVE CARE
The degree of postoperative immobilization depends on numerous factors, including the mode of fracture stabilization, the quality of the bone for internal fixation, the stability of the fixation, and the management of any associated soft tissue injuries that were addressed during the arthroscopic evaluation.Immediate range of motion of the digits and wrist is initiated in patients with volar plate fixation with good bone stock and solid fixation.In patients with soft osteopenic bone with volar plate fixation, digital range-of-motion exercises are initiated immediately, but wrist range of motion is delayed approximately 3 to 4 weeks to permit some fracture healing.Soft bone may collapse around the rigid plate.In patients without metaphyseal comminution treated by arthroscopically assisted stabilization with cannulated screws, range of motion is initiated as the patient tolerates.In patients treated with percutaneous K-wires, the wrist is immobilized until the wires are removed, usually 4 to 6 weeks after surgery.A patient with an unstable DRUJ is treated by TFCC repair or ulnar styloid reduction and fixation is restricted from pronation and supination for 2 to 4 weeks.
OUTCOMES
The literature is relatively sparse regarding the results of arthroscopically assisted fixation of displaced intra-articular distal radius fractures. 9,10,12,13,22,27,30A comparison study of 12 open and 12 arthroscopic reductions of comminuted AO types VII and VIII fractures of the distal radius found that the arthroscopic group had increased range of motion as compared to the open stabilization group. 32A second comparison study of 38 patients who underwent arthroscopically assisted fixation compared to open reduction found the arthroscopically assisted group had better results and improved range of motion. 3 One study compared 15 patients with arthroscopically assisted fixation to 15 patients who underwentclosed reduction and external fixation. 30 In this study, there were 10 tears of the TFCC in the group that underwent arthroscopic reduction, of which 7 were peripheral and repaired. There were no signs of DRUJ instability at final follow-up visit. In the 15 patients who underwent stabilization by external fixation alone, 4 patients had continued complaints of instability of the distal radial joint, very possibly the result of undiagnosed and untreated TFCC tears.Ono et al 27 evaluated articular gaps and step-offs following open reduction and plating for intra-articular distal radius fractures without arthroscopic assistance. They evaluated 70 patients prospectively, recording both gaps and step-offs from CT preoperatively and the arthroscope postoperatively. The authors noted 40 patients had a gap of greater than or equal to 1 mm and 15 had a step-off of greater than or equal to 1 mmpostoperatively. 27
COMPLICATIONS
Failure of fixationLate settling of the fracture despite fixation Flexor and extensor tendon irritationPainful metal requiring removalP.273Neuromas of the dorsal sensory branch of the radial and ulnar nerves Carpal tunnel syndromeReflex sympathetic dystrophy Wrist and hand stiffness
REFERENCES
- Abe Y, Yoshida K, Tominaga Y. Less invasive surgery with wrist arthroscopy for distal radius fractures. J Orthop Sci 2013;18:398-404.
- Arora R, Gabl M, Gschwentner M, et al. A comparative study of clinical and radiologic outcomes of unstable colles type distal radius fractures in patients older than 70 years: nonoperative treatment versus volar locking plating. J Orthop Trauma 2009;23(4):237-242.
- Arora R, Lutz M, Deml C, et al. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am 2011;93(23):2146-2453.
- Bradway JK, Amadio PC, Cooney WP. Open reduction and internal fixation of displaced comminuted intraarticular fractures of the distal end of the radius. J Bone Joint Surg Am 1989;71(6):839-847.
- del Piñal F, Cagigal L, García-Bernal FJ, et al. Arthroscopically guided osteotomy for management of intraarticular distal radius malunions. J Hand Surg Am 2010;35(3):392-397.
- del Piñal F, García-Bernal FJ, Delgado J, et al. Correction of malunited intra-articular distal radius fractures with an inside-out osteotomy technique. J Hand Surg Am 2006;31(6):1029-1034.
- del Piñal F, García-Bernal FJ, Pisani D, et al. Dry arthroscopy of the wrist: surgical technique. J Hand Surg Am 2007;32(1):119-123.
- del Piñal F, Klausmeyer M, Thams C, et al. Arthroscopic resection arthroplasty for malunited intra-articular distal radius fractures. J Hand Surg Am 2012;37(12):2447-2455.
- Doi K, Hattori T, Otsuka K, et al. Intra-articular fractures of the distal aspect of the radius arthroscopically assisted reduction compared with open reduction and internal fixation. J Bone Joint Surg Am 1999;81(8):1093-1110.
- Edwards CC II, Haraszti CJ, McGillivary GR, et al. Intra-articular distal radius fractures: arthroscopic assessment of radiographically assisted reduction. J Hand Surg Am 2001;26(6):1036-1041.
- Fernandez DL, Geissler WB. Treatment of displaced articular fractures of the radius. J Hand Surg Am 1991;16:375-384.
- Geissler WB. Arthroscopically assisted reduction of intra-articular fractures of the distal radius. Hand Clin 1995;11:19-29.
- Geissler WB. Intra-articular distal radius fractures: the role of arthroscopy? Hand Clin 2005;21:407-416.
- Geissler WB, Freeland AE. Arthroscopically assisted reduction of intraarticular distal radial fractures. Clin Orthop Relat Res 1996;(327):125-134.
- Geissler WB, Freeland AE, Savoie FH, et al. Intracarpal soft-tissue lesions associated with an intraarticular fracture of the distal end of the radius. J Bone Joint Surg Am 1996;78(3):357-365.
- Geissler WB, Savoie FH. Arthroscopic techniques of the wrist. Mediguide Orthop 1992;11:1-8.
- Hanker GJ. Wrist arthroscopy in distal radius fractures. Proceedings of the Arthroscopy Association North America Annual Meeting, Albuquerque, NM, October 7-9, 1993.
- Hixon ML, Fitzrandolph R, McAndrew M, et al. Acute ligamentous tears of the wrist associated with Colles fractures. Proceedings of the Annual Meeting of the American Society for Surgery of the Hand, Baltimore, 1989.
- Hollingworth R, Morris J. The importance of the ulnar side of the wrist in fractures of the distal end of the radius. Injury 1976;7: 263-266.
- Knirk JL, Jupiter JB. Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg Am 1986;68(5):647-659.
- Lafontaine M, Hardy D, Delince P. Stability assessment of distal radius fractures. Injury 1989;20:208-210.
- Levy HJ, Glickel SZ. Arthroscopic assisted internal fixation of intraarticular wrist fractures. Arthroscopy 1993;9:122-124.
- Lindau T. Treatment of injuries to the ulnar side of the wrist occurring with distal radial fractures. Hand Clin 2005;21:417-425.
- Melone CP Jr. Articular fractures of the distal radius. Orthop Clin North Am 1984;15:217-236.
- Mohanti RC, Kar N. Study of triangular fibrocartilage of the wrist joint in Colles fracture. Injury 1979;11:321-324.
- Mudgal CS, Jones WA. Scapholunate diastasis: a component of fractures of the distal radius. J Hand Surg Br 1990;15:503-505.
- Ono H, Katayama T, Furuta K, et al. Distal radial fracture arthroscopic intraarticular gap and step-off measurement after open reduction and internal fixation with a volar locked plate. J Orthop Sci 2012;17(4):443-449.
- Oqawa T, Tanaka T, Yanai T, et al. Analysis of soft tissue injuries associated with distal radius fractures. BMC Sports Sci Med Rehabil 2013;5(1):19.
- Ruch DS, Vallee J, Poehling GG, et al. Arthroscopic reduction versus fluoroscopic reduction in the management of intra-articular distal radius fractures. Arthroscopy 2004;20:225-230.
- Short WH, Palmer AK, Werner FW, et al. A biomechanical study of distal radial fractures. J Hand Surg Am 1987;12:529-534.
- Stewart NJ, Berger RA. Comparison study of arthroscopic as open reduction of comminuted distal radius fractures. Abstract. Presented at the 53rd Annual Meeting of the American Society for Surgery of the Hand, January 11, 1998, Scottsdale, AZ.
- Trumble TE, Schmitt SR, Vedder NB. Factors affecting functional outcome of displaced intra-articular distal radius fractures. J Hand Surg Am 1994;19:325-340.
