INTRODUCTION TO ADVANCED CARPAL SALVAGE
The evolution of wrist arthroscopy has revolutionized the management of complex carpal pathology. Arthroscopic Proximal Row Carpectomy (APRC) represents a sophisticated, minimally invasive evolution of the traditional open proximal row carpectomy. By excising the scaphoid, lunate, and triquetrum entirely through arthroscopic portals, surgeons can convert a complex, arthritic intercalated segment into a simplified, functional hinge joint where the capitate articulates directly with the lunate fossa of the distal radius.
Compared to open techniques, APRC preserves the critical dorsal radiocarpal ligaments and the dorsal capsule, significantly reducing postoperative stiffness, minimizing proprioceptive loss, and accelerating functional rehabilitation.
Additionally, this guide will cover the Matti-Russe Technique, a foundational volar bone-grafting procedure utilized for the management of recalcitrant carpal scaphoid nonunions, ensuring a comprehensive understanding of both carpal salvage and reconstructive joint preservation.
ARTHROSCOPIC PROXIMAL ROW CARPECTOMY (WEISS ET AL. TECHNIQUE)
Biomechanical Rationale
The proximal carpal row functions as an intercalated segment between the rigid distal radius and the tightly bound distal carpal row. In conditions such as Scapholunate Advanced Collapse (SLAC), Scaphoid Nonunion Advanced Collapse (SNAC), or advanced Kienböck's disease, the kinematics of this segment are destroyed, leading to progressive radiocarpal and midcarpal arthrosis.
By removing the proximal row, the head of the capitate is allowed to migrate proximally and seat within the lunate fossa. Because the radius of curvature of the capitate head closely matches that of the lunate fossa, a congruent, stable articulation is formed.
Surgical Warning:
The absolute prerequisite for a successful proximal row carpectomy—whether open or arthroscopic—is the presence of pristine, healthy articular cartilage on both the head of the capitate and the lunate fossa of the distal radius. If advanced chondromalacia or eburnation is present in either of these areas, APRC is strictly contraindicated, and a four-corner fusion or total wrist arthrodesis must be performed instead.
Indications and Contraindications
Indications:
* Stage II SLAC wrist (arthritis limited to the radioscaphoid joint).
* Stage II SNAC wrist.
* Advanced Kienböck’s disease (Lichtman Stage IIIA or IIIB) with a preserved capitate.
* Chronic perilunate dislocations unamenable to reconstruction.
Contraindications:
* Stage III SLAC/SNAC wrist (involvement of the capitolunate joint).
* Degenerative changes in the lunate fossa.
* Inflammatory arthropathies (e.g., Rheumatoid Arthritis) due to the risk of progressive ulnar translation.
* Severe ulnar variance precluding proper capitate seating.
Preoperative Planning and Positioning
- Imaging: Standard posteroanterior (PA), lateral, and scaphoid views are mandatory. A preoperative MRI or diagnostic arthroscopy is highly recommended to definitively assess the cartilage status of the capitate head and lunate fossa.
- Anesthesia: Regional block (supraclavicular or axillary) combined with intravenous sedation or general anesthesia.
- Positioning: The patient is placed supine with the operative arm extended on a hand table. A well-padded proximal arm tourniquet is applied.
- Traction: The hand is placed in a standardized wrist traction tower using sterile finger traps on the index and long fingers. Approximately 10 to 15 pounds of longitudinal traction is applied to distract the radiocarpal and midcarpal joints.
Surgical Portals and Anatomy
Thorough knowledge of dorsal wrist portals is essential for safe instrument navigation and complete carpal excision.
* 3-4 Portal: Located between the extensor pollicis longus (EPL) and extensor digitorum communis (EDC). Used primarily for radiocarpal viewing.
* 4-5 Portal: Located between the EDC and extensor digiti minimi (EDM). Used for radiocarpal working.
* 6R and 6U Portals: Located radial and ulnar to the extensor carpi ulnaris (ECU), respectively.
* Midcarpal Radial (MCR) Portal: Located approximately 1 cm distal to the 3-4 portal, in the palpable soft spot between the capitate, scaphoid, and lunate.
* Midcarpal Ulnar (MCU) Portal: Located 1 cm distal to the 4-5 portal, between the capitate, hamate, lunate, and triquetrum.
* Scaphotrapezial-trapezoid (STT) Portal: Located just distal to the scaphoid tubercle, radial to the FCR tendon.
Step-by-Step Surgical Technique
1. Diagnostic Arthroscopy
- Establish the 3-4 and 4-5 portals to carry out a routine radiocarpal examination. Assess the radiocarpal ligaments, the triangular fibrocartilage complex (TFCC), and the articular surfaces.
- Transition to the midcarpal joint using the MCR and MCU portals. Confirm that the cartilage on the proximal pole of the capitate is intact and free of significant degenerative changes.
2. Initial Scaphoid Decortication
- Introduce a small joint arthroscopic burr or aggressive shaver into the midcarpal joint through the midcarpal radial (MCR) portal.
- Place the arthroscope in the midcarpal ulnar (MCU) portal for optimal viewing of the scapholunate interval.
- Begin by using the burr or shaver to decorticate the medial corner of the scaphoid at the midcarpal scapholunate joint.
Clinical Pearl:
During the initial decortication of the scaphoid, the burr is in close proximity to the capitate. Maintain the burr's cutting window directed radially and volarly at all times. Take extreme care not to inadvertently score or injure the articular cartilage of the head of the capitate, as this will compromise the final functional outcome.
3. Scaphoid Excision
- Once an adequate portion of the medial corner of the scaphoid is removed, slightly enlarge the MCR portal using careful blunt dissection with a mosquito hemostat to accommodate larger instruments.
- Introduce a 4.0-mm hooded burr into the midcarpal joint. The hood provides a protective shield against the capitate.
- Proceed to remove the scaphoid systematically. The optimal trajectory for scaphoid removal is from ulnar to radial and distal to proximal.
- To access the distal pole of the scaphoid, utilize the STT portal while viewing through the MCR portal.

FIGURE 69-37A: Arthroscopic proximal row carpectomy. Initial removal of the distal ulnar pole of the scaphoid using a hooded burr, carefully avoiding the capitate head.
4. Lunate and Triquetrum Excision
- After complete scaphoid excision, reposition the arthroscope into the STT or MCR portal to view the remaining proximal row from a radial perspective.
- Place the 4.0-mm burr into an enlarged MCR or MCU portal.
- Sequentially remove the lunate, working from distal to proximal.
- Follow with the excision of the triquetrum, again working from distal to proximal. Ensure that the volar radiocarpal ligaments (which attach to the lunate) are preserved to prevent volar subluxation of the carpus postoperatively.

FIGURE 69-37B: The entire proximal row (scaphoid, lunate, and triquetrum) has been completely excised, leaving a void for the capitate to migrate proximally.
5. Debridement and Fluoroscopic Confirmation
- Under direct arthroscopic vision, introduce a fine synovial rongeur or grasping forceps to meticulously remove any tiny fragments of bone or cartilage that remain adherent to the volar or dorsal capsule. Retained fragments can act as loose bodies, causing mechanical catching and pain.
- Bring in the fluoroscopy unit (C-arm) to confirm the complete excision of the proximal row carpectomy. Ensure no osseous remnants of the scaphoid tuberosity or triquetrum remain.
6. Capitate Seating and Radial Styloidectomy
- Release the longitudinal traction from the tower.
- Use both arthroscopy and fluoroscopy to confirm the proper seating of the head of the capitate directly into the lunate fossa of the distal radius.

FIGURE 69-37C: After the release of traction, the capitate head is shown smoothly seated within the lunate fossa, establishing the new radiocarpal articulation.
- Passively deviate the wrist radially under fluoroscopic visualization. If sufficient radiocarpal impaction is observed between the radial styloid and the trapezium or the base of the capitate, a concomitant arthroscopic radial styloidectomy is indicated.
- To perform the styloidectomy, place the burr in the 1-2 portal and the arthroscope in the 3-4 portal. Resect the styloid transversely to remove the radial edge of the lunate fossa, taking care not to detach the radioscaphocapitate (RSC) ligament.
7. Closure
- Thoroughly irrigate the joint to remove all bone debris.
- Repair the dorsal capsule if it was significantly violated during portal enlargement, though standard arthroscopic portals typically require only skin closure.
- Close the skin with non-absorbable sutures (e.g., 4-0 nylon).
Postoperative Rehabilitation Protocol
Because APRC preserves the dorsal capsule and extrinsic ligaments, rehabilitation can be tailored based on the surgeon's assessment of capsular integrity and patient compliance. Two primary pathways exist:
Pathway A: Accelerated Protocol (Preferred for strict arthroscopic cases)
* Days 0-2: A bulky compressive dressing and a volar resting splint are applied in the operating room. The wrist is immobilized in slight extension. Immediate active range of motion (ROM) of the fingers, thumb, elbow, and shoulder is mandated to prevent tendon adhesions and reduce edema.
* Day 2: The bulky bandage is removed. A custom-molded, removable volar splint is applied for comfort. Early active and gentle passive range of motion of the wrist is encouraged out of the splint.
* Weeks 2-6: Sutures are removed at 10-14 days. The patient is transitioned to formal physical therapy. Return to light activities of daily living (ADLs) is allowed within the limits of comfort.
* Weeks 6+: Splinting is discontinued. Progressive strengthening begins.
Pathway B: Conservative Protocol (If capsular repair was required)
* Weeks 0-3: Continuous immobilization in a short-arm cast or rigid splint in slight extension.
* Weeks 3-6: The rigid immobilization is transitioned to a removable splint. Progressive active and passive wrist exercises are initiated under the guidance of a hand therapist.
* Weeks 6+: Splinting is discontinued, and strengthening exercises commence.
MATTI-RUSSE TECHNIQUE FOR SCAPHOID NONUNION
While APRC is a salvage procedure for advanced arthritis, isolated scaphoid nonunions without secondary arthritic changes are best managed with joint-preserving reconstructive techniques. The Matti-Russe technique is a classic, highly effective volar approach for bone grafting ununited fractures of the carpal scaphoid, particularly when the nonunion is located in the middle or distal third and is associated with volar intercalated segment instability (VISI) or cystic resorption.
Surgical Principles
The Matti-Russe procedure utilizes a volar approach to excavate the necrotic, fibrous tissue at the nonunion site, creating a vascularized trough. This trough is then densely packed with autologous corticocancellous bone graft, typically harvested from the iliac crest or the distal radius, to restore scaphoid length, correct the intrascaphoid angle, and promote osteogenesis.
Surgical Technique
-
Incision and Exposure:
- A longitudinal or slightly curved volar incision is made over the course of the flexor carpi radialis (FCR) tendon, extending across the radiocarpal joint.
- The FCR tendon sheath is incised, and the tendon is retracted ulnarly to protect the median nerve.
- The floor of the FCR sheath (which constitutes the volar radiocarpal capsule) is incised longitudinally to expose the underlying scaphoid.
-
Preparation of the Nonunion Site:
- The nonunion site is identified. A small curette or high-speed burr is used to meticulously excavate all fibrous tissue, sclerotic bone, and necrotic debris from both the proximal and distal fragments.
- The excavation continues until healthy, bleeding cancellous bone is encountered (the "paprika sign"). This creates an ovoid cavity or trough spanning the nonunion.
-
Graft Harvesting and Placement:
- A corticocancellous bone graft is harvested.
- The wrist is placed in ulnar deviation and slight extension to open the scaphoid defect and correct any humpback deformity.
- The graft is contoured to fit the excavated trough precisely. The cortical portion of the graft can be positioned volarly to provide structural support and maintain the corrected scaphoid length, while the cancellous portion fills the void to promote rapid incorporation.
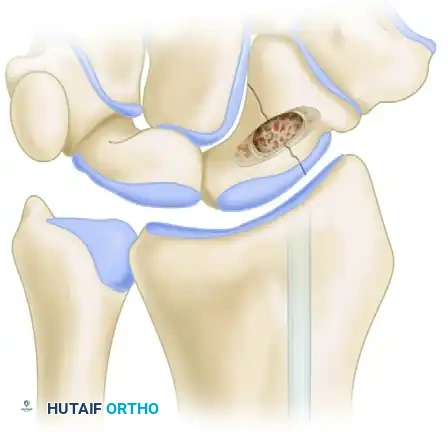
FIGURE 69-38 (Overview): Matti-Russe technique of bone grafting for nonunion of the carpal scaphoid. The volar approach utilizes the interval of the flexor carpi radialis to access the scaphoid.

FIGURE 69-38 (Detail): Close-up view of the corticocancellous graft firmly impacted into the excavated trough of the scaphoid, bridging the proximal and distal poles.
- Fixation and Closure:
- While the original Matti-Russe technique relied solely on the press-fit stability of the graft and cast immobilization, modern iterations frequently supplement the construct with headless compression screws or Kirschner wires to provide rigid internal fixation.
- The volar capsule is carefully repaired, followed by routine skin closure.
- Postoperatively, the wrist is immobilized in a thumb spica cast until radiographic union is confirmed, typically between 8 to 12 weeks depending on the rigidity of the internal fixation used.
Surgical Pitfall:
Failure to adequately correct the "humpback" (flexion) deformity of the scaphoid prior to graft insertion will result in a malunited scaphoid. This alters carpal kinematics, leading to a loss of wrist extension and eventual midcarpal arthrosis, ultimately requiring salvage procedures such as the APRC detailed above.
📚 Medical References
- Proximal row carpectomy in arthrogrypotic wrist deformity, J Hand Surg 12A:523, 1987.
- Widman RF, Do TT, Burke SW: Radical soft-tissue release of the arthrogrypotic clubfoot, J Pediatr Orthop 14B:111, 2005.
- Williams PF: The management of arthrogryposis, Orthop Clin North Am 6:967, 1978.
- Williams PF: Management of upper limb problems in arthrogryposis, Clin Orthop Relat Res 194:60, 1985.
- Williams PF: Personal communication, 1985.
- Wynne-Davies RW, Williams PF, O’Connor JBF: The 1960’s epidemic of arthrogryposis multiplex congenita, J Bone Joint Surg 63B:76, 1981.
- Yingsakmongkol W, Kumar SJ: Scoliosis in arthrogryposis multiplex congenita: results after nonsurgical and surgical treatment, J Pediatr Orthop 20:656, 2000.
- Brachial Plexus Allende CA, Gilbert A: Forearm supination deformity after obstetric paralysis, Clin Orthop Relat Res 426:206, 2004.
- Al-Qattan MM: Latissimus dorsi transfer for external rotation weakness of the shoulder in obstetric
