Comprehensive Introduction and Patho-Epidemiology
Arthroscopic osteocapsular arthroplasty combined with glenoidplasty represents a sophisticated, joint-preserving surgical intervention designed for a highly specific demographic: the young, active patient suffering from advanced glenohumeral degenerative joint disease (DJD). Historically, orthopedic surgeons faced a difficult clinical dilemma when managing patients under the age of fifty-five who presented with debilitating shoulder osteoarthritis. Total shoulder arthroplasty (TSA), while highly successful in older, low-demand populations, carries an unacceptably high rate of premature glenoid component loosening and failure in young, heavy laborers or high-impact athletes. Consequently, arthroscopic interventions have evolved from simple palliative joint lavage and debridement to comprehensive, biomechanically driven reconstructions aimed at restoring glenohumeral kinematics, maximizing range of motion, and providing durable symptomatic relief without burning bridges for future arthroplasty.
The pathogenesis of glenohumeral osteoarthritis is a complex, multifactorial cascade involving mechanical wear, biochemical degradation, and adaptive structural changes. Unlike weight-bearing joints such as the knee or hip, the shoulder is a highly mobile, unconstrained joint where stability relies heavily on the intricate balance of the dynamic rotator cuff musculature and the static capsuloligamentous complex. As articular cartilage undergoes progressive fibrillation and full-thickness loss, the joint experiences altered mechanotransduction. This abnormal loading stimulates subchondral bone sclerosis and the formation of marginal osteophytes. These osteophytes, particularly those located at the inferior humeral neck (the "goat's beard") and the inferior glenoid margin, physically impinge during arm elevation and rotation, leading to profound motion loss and secondary capsular contracture.
Furthermore, the altered kinematics in the osteoarthritic shoulder frequently lead to asymmetric posterior glenoid wear. As the humeral head subluxates posteriorly—often driven by a tight anterior capsule and subscapularis contracture—eccentric loading occurs on the posterior aspect of the glenoid vault. Over time, this eccentric wear pattern creates a biconcave glenoid morphology, classically described in the Walch classification system as a B2 glenoid. The native anterior glenoid (paleoglenoid) remains relatively preserved, while a newly eroded posterior articulation (neoglenoid) forms. This biconcavity acts as a mechanical block to concentric reduction of the humeral head, exacerbating static posterior subluxation and accelerating the degenerative cycle.
The objective of an arthroscopic osteocapsular arthroplasty and glenoidplasty is not to halt or reverse this underlying biological degeneration, but rather to meticulously re-engineer the joint's mechanical environment. By performing a radical capsular release, excising impinging marginal osteophytes, and systematically burring down the paleoglenoid to re-establish a single, concentric concavity, the surgeon can recenter the humeral head and restore a functional, pain-free arc of motion. This "intraoperative masterclass" demands a profound understanding of three-dimensional anatomy, precise portal placement, and advanced arthroscopic burring techniques to safely navigate the perilabral and inferior capsular spaces while protecting vital neurovascular structures.
Detailed Surgical Anatomy and Biomechanics
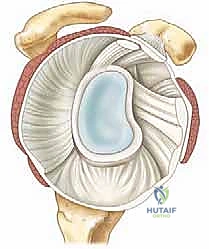
A rigorous command of glenohumeral surgical anatomy and biomechanics is the absolute foundation for executing a safe and effective osteocapsular arthroplasty. The glenohumeral joint is inherently unstable, often likened to a golf ball sitting on a tee. The humeral head possesses an articular surface area approximately three to four times larger than that of the glenoid fossa. The proximal humerus is characterized by a head-shaft angle of approximately 130 degrees and is typically retroverted about 30 degrees relative to the transepicondylar axis of the distal humerus. The native glenoid is a shallow, pear-shaped socket that is typically retroverted between 2 and 5 degrees and has a slight superior inclination.
To compensate for this bony mismatch, the joint relies heavily on the fibrocartilaginous labrum and the complex capsuloligamentous network. The labrum functions as a critical static stabilizer by acting as a "chock block" and significantly deepening the glenoid vault—increasing its superoinferior depth by an average of 9 mm and its anteroposterior depth by 5 mm. Furthermore, the labrum serves as the attachment site for the glenohumeral ligaments (superior, middle, and inferior). The inferior glenohumeral ligament (IGHL) complex, comprising the anterior band, posterior band, and the axillary pouch, is the primary restraint to anterior, posterior, and inferior translation when the arm is in an abducted and externally rotated position. In the setting of osteoarthritis, this capsule becomes profoundly thickened, fibrotic, and contracted, tethering the humeral head and forcing it out of concentric alignment.
Biomechanically, the stability of the glenohumeral joint during active motion is governed by the principle of "concavity compression." The coordinated contraction of the rotator cuff muscles compresses the humeral head directly into the concave glenoid socket, resisting shear forces. However, in a Walch B2 osteoarthritic glenoid, the presence of the central osseous ridge dividing the paleoglenoid and neoglenoid disrupts this concavity compression mechanism. The humeral head preferentially rests in the retroverted neoglenoid. When the patient attempts to elevate or rotate the arm, the humeral head is forced to ride up and over the central ridge, resulting in painful crepitus, mechanical catching, and further labral and chondral destruction.
Understanding the intimate relationship of the axillary nerve to the inferior capsule is paramount during the capsular release and inferior osteophyte excision phases of this procedure. The axillary nerve exits the axilla through the quadrangular space, coursing directly inferior to the capsule of the glenohumeral joint. Cadaveric studies have demonstrated that the nerve lies, on average, merely 10 to 14 mm from the inferior glenoid rim at the 6 o'clock position. In the presence of large inferior osteophytes and a contracted capsule, this safe zone can be significantly distorted and reduced. When the arm is placed in traction and abduction (as in the lateral decubitus position), the nerve is tensioned and drawn even closer to the inferior capsule. Therefore, all capsular releases and burring in the inferior recess must be performed under direct, meticulous visualization, maintaining the cutting instruments strictly within the joint space and directed away from the axillary pouch floor.
Exhaustive Indications and Contraindications
Patient selection is arguably the most critical determinant of success for arthroscopic osteocapsular arthroplasty and glenoidplasty. This procedure is not a universal solution for all shoulder arthritis; rather, it is a highly targeted intervention for a specific clinical profile. The ideal candidate is a chronologically or physiologically young patient (typically under 50 to 55 years of age) who presents with moderate to severe glenohumeral osteoarthritis and exhibits a high demand for physical activity. These are often heavy manual laborers, weightlifters, or high-impact athletes who would rapidly wear out or loosen the polyethylene glenoid component of a traditional total shoulder arthroplasty.
Clinically, these patients present with deep, aching shoulder pain that is refractory to comprehensive non-operative management, including physical therapy, non-steroidal anti-inflammatory drugs (NSAIDs), and intra-articular corticosteroid or biologic injections. A hallmark physical exam finding is painful crepitus during active and passive glenohumeral motion, accompanied by a significant, symmetric loss of range of motion. Loss of internal rotation up the back and diminished forward elevation are particularly prominent due to the combination of posterior capsular contracture and inferior osteophyte impingement. Importantly, the patient must have an intact and functioning rotator cuff, as the success of the glenoidplasty relies heavily on the dynamic stabilizing forces of the cuff to maintain the humeral head in the newly recontoured glenoid concavity.
Contraindications must be strictly respected to avoid early catastrophic failure. Absolute contraindications include active joint infection, severe inflammatory arthropathies (such as advanced rheumatoid arthritis) where the primary pathology is synovial driven rather than mechanical, and massive, irreparable rotator cuff tears. In the setting of a deficient rotator cuff, the joint lacks the necessary concavity compression to stabilize the head, and a glenoidplasty will likely fail to provide lasting relief; these patients are better served by a reverse total shoulder arthroplasty (RTSA) if age-appropriate. Relative contraindications include advanced age with low physical demands, where a standard TSA provides superior, more predictable, and longer-lasting pain relief. Additionally, extreme glenoid bone loss or severe medialization that would preclude future arthroplasty is a relative contraindication, as the surgeon must carefully weigh the amount of bone removed during glenoidplasty against the bone stock required for eventual TSA conversion.
| Clinical Parameter | Indications for AOCA & Glenoidplasty | Relative Contraindications | Absolute Contraindications |
|---|---|---|---|
| Patient Age | Young (< 50-55 years) | Older (> 65 years) with low demands | N/A |
| Activity Level | High demand, heavy manual labor, elite sports | Sedentary lifestyle | N/A |
| Pathology | Moderate to severe OA, Walch A or B1/B2 glenoid | Walch C glenoid (dysplastic), severe bone loss | Active joint infection, Neuropathic joint |
| Rotator Cuff | Intact and functional | Reparable partial or small full-thickness tear | Massive, irreparable cuff tear (pseudoparalysis) |
| Prior Treatments | Refractory to >6 months conservative care | Minimal prior conservative management | N/A |
| Patient Goals | Delay arthroplasty, maintain heavy lifting ability | Desires definitive, immediate pain elimination | Unwillingness to comply with aggressive rehab |
Pre-Operative Planning, Templating, and Patient Positioning
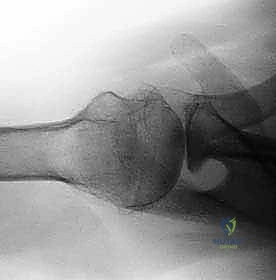
Thorough preoperative planning, heavily reliant on advanced imaging, is non-negotiable for this complex procedure. The standard radiographic shoulder series must include a true anteroposterior (AP) view in the scapular plane (Grashey view), a scapular Y lateral, and an axillary lateral view. The true AP view is essential for evaluating the extent of joint space narrowing, the presence of subchondral cysts, and the size of the inferior humeral osteophyte (the "goat's beard").
The axillary lateral view is arguably the most critical plain radiograph, as it provides the initial assessment of glenoid version, posterior wear, and static posterior subluxation of the humeral head.
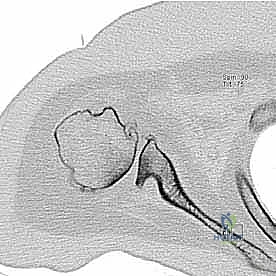
While plain radiographs provide a baseline, a non-contrast Computed Tomography (CT) scan is the gold standard for preoperative templating in glenoidplasty. The axial, coronal, and sagittal 2D slices allow for precise measurement of glenoid retroversion and the depth of the posterior wear defect.

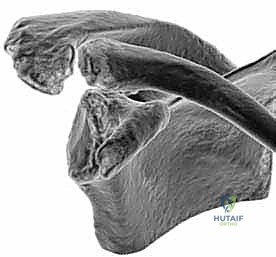
Furthermore, three-dimensional (3D) CT reconstructions with digital subtraction of the humeral head are invaluable. These 3D models allow the surgeon to virtually rotate the scapula and directly visualize the biconcave glenoid morphology from the perspective of the intended arthroscopic portals. This spatial understanding dictates exactly how much of the anterior paleoglenoid must be resected to match the depth of the posterior neoglenoid, thereby re-establishing a single, concentric articular surface.
Magnetic Resonance Imaging (MRI) is routinely obtained to evaluate the integrity of the rotator cuff musculature, the biceps tendon, and the labrum. While CT is superior for bone, MRI is critical for ensuring the patient does not have a concomitant massive rotator cuff tear that would contraindicate the joint-preserving approach.
On the day of surgery, anesthesia typically consists of a regional interscalene nerve block combined with general endotracheal anesthesia. The interscalene block is crucial for preemptive analgesia, minimizing intraoperative narcotic requirements, and facilitating the aggressive early postoperative range of motion therapy required after capsular release. Patient positioning is a matter of surgeon preference, utilizing either the beach-chair or the lateral decubitus position. However, for extensive osteocapsular arthroplasty and glenoidplasty, the lateral decubitus position is highly advantageous.

The patient is placed in the lateral decubitus position on a beanbag, with all bony prominences meticulously padded. The operative arm is suspended in a specialized traction device, typically utilizing 10 to 15 pounds of weight. The arm is positioned in approximately 45 to 60 degrees of abduction and 15 to 20 degrees of forward flexion. This traction vector distracts the glenohumeral joint, opening the tightly contracted osteoarthritic space and providing the surgeon with unparalleled access to the inferior capsule and the inferior glenoid margin. Prior to prepping and draping, a thorough Examination Under Anesthesia (EUA) is performed to document the true passive range of motion, noting specific deficits in internal rotation, external rotation, and elevation, which will guide the extent of the intraoperative capsular release.
Step-by-Step Surgical Approach and Glenoidplasty Technique
The surgical execution of an arthroscopic osteocapsular arthroplasty requires a systematic, disciplined approach, beginning with precise portal placement. Due to the distorted anatomy and capsular contracture inherent in severe OA, standard portal locations often need to be modified.
The initial posterior viewing portal is typically established slightly more inferior and lateral than the standard "soft spot" portal. This inferiorized posterior portal provides a superior trajectory for visualizing the anterior glenoid neck and the inferior axillary pouch, which are critical zones for osteophyte resection and capsular release. An anterior portal is then established under direct intra-articular visualization using an outside-in spinal needle localization technique. This portal is placed through the rotator interval, slightly superior to the subscapularis tendon, and again, often slightly more inferior than a standard anterior portal to facilitate the angle of approach for the burr.
Once access is achieved, a comprehensive diagnostic arthroscopy is performed, systematically evaluating the joint using a 15-point assessment. The surgeon will typically encounter a hostile intra-articular environment characterized by florid synovitis, extensive chondral delamination, multiple loose bodies, and a profoundly thickened, hyperemic capsule.

The first operative step is a thorough joint lavage and synovectomy using a motorized shaver and radiofrequency ablation wand. All loose bodies, which frequently hide in the axillary pouch or the subscapularis recess, must be meticulously identified and removed. Following the synovectomy, the surgeon addresses the biceps tendon. In advanced OA, the long head of the biceps is almost universally frayed, subluxated, or acting as a pain generator. A routine arthroscopic biceps tenodesis or tenotomy is performed to eliminate this source of anterior shoulder pain.
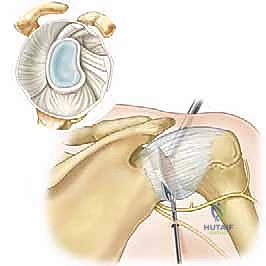
The procedure then transitions to the osteocapsular arthroplasty phase. The goal is to decompress the joint by removing the impingement-causing marginal osteophytes. Using a 4.0-mm or 5.5-mm hooded spherical burr introduced via the anterior portal, the surgeon systematically resects the inferior humeral osteophyte.

The burr is carefully swept along the anatomic neck of the humerus, restoring the normal spherical contour of the humeral head. Extreme caution must be exercised to avoid iatrogenic notching of the true articular surface or penetrating too deeply into the inferior capsule. Following humeral osteophyte resection, attention is turned to the glenoid osteophytes, particularly those located at the inferior and posterior margins.
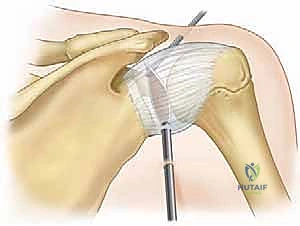
Concurrent with osteophyte resection, a comprehensive capsular release is executed to restore glenohumeral kinematics. Using a radiofrequency device, the contracted anterior, inferior, and posterior capsules are sequentially released directly off the glenoid rim.

The release begins anteriorly at the rotator interval, extending inferiorly through the middle and inferior glenohumeral ligaments. As the dissection reaches the 6 o'clock position (the axillary pouch), the surgeon must remain intimately close to the bony glenoid margin to avoid thermal or mechanical injury to the axillary nerve, which lies just millimeters away. The release is continued posteriorly and superiorly until the humeral head can be freely translated within the joint space.
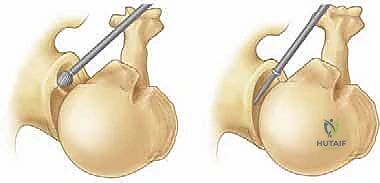
The final, and most technically demanding, phase of the procedure is the glenoidplasty. In the setting of a Walch B2 biconcave glenoid, the objective is to perform concentric reaming (via a high-speed burr) to eliminate the central osseous ridge and create a single, unified concavity.
The burr is utilized to systematically take down the prominent anterior paleoglenoid. The surgeon must constantly reference the depth of the posterior neoglenoid, using it as the template for the final recontoured surface. The burring is performed in a sweeping, painting motion, gradually blending the anterior and posterior surfaces.
The goal is not to completely correct the retroversion to 0 degrees—which would require excessive bone resection and compromise future arthroplasty—but rather to eliminate the mechanical block of the biconcavity and recenter the humeral head. Once the glenoidplasty is complete, the joint is thoroughly irrigated to remove all bone debris, and a final dynamic examination is performed under arthroscopic visualization to confirm concentric reduction and the absence of impingement throughout a full range of motion.
Complications, Incidence Rates, and Salvage Management
While arthroscopic osteocapsular arthroplasty and glenoidplasty offer a valuable joint-preserving option, the procedure is technically demanding and carries a distinct profile of potential complications. The most devastating intraoperative complication is iatrogenic injury to the axillary nerve. Given the nerve's intimate proximity to the inferior capsule—often drawn even closer by capsular contracture and lateral decubitus traction—errant placement of a radiofrequency wand or an unhooded burr during the inferior capsular release or osteophyte resection can result in permanent deltoid paralysis. The incidence of clinically significant axillary nerve injury is exceedingly low in the hands of experienced arthroscopists (less than 1%), but the risk is ever-present. Prevention relies on meticulous visualization, maintaining instruments strictly on the intra-articular side of the capsule, and avoiding plunging into the axillary recess.
Another significant technical complication is inadequate or excessive bone resection during the glenoidplasty. Inadequate resection leaves a residual biconcavity, failing to recenter the humeral head and resulting in persistent pain, mechanical catching, and early procedural failure. Conversely, over-resection of the anterior paleoglenoid can significantly medialise the joint line, potentially destabilizing the shoulder anteriorly and, more critically, depleting the vital glenoid bone stock required for future total shoulder arthroplasty. The surgeon must strike a delicate balance, removing just enough bone to restore a single concavity while preserving maximum bone volume.
Postoperative complications include stiffness, recurrent pain, and infection. Despite aggressive intraoperative capsular release, some patients may develop recurrent adhesive capsulitis, particularly if they are non-compliant with the early, aggressive rehabilitation protocol. Infection is rare in shoulder arthroscopy (typically <0.5%), but given the extensive bony work and fluid extravasation, meticulous sterile technique and appropriate perioperative antibiotic prophylaxis are mandatory.
When arthroscopic osteocapsular arthroplasty eventually fails—and it is important to counsel patients that this is often a time-buying procedure rather than a permanent cure—the salvage management is conversion to a shoulder arthroplasty. If the rotator cuff remains intact and sufficient glenoid bone stock was preserved, a standard anatomic Total Shoulder Arthroplasty (TSA) can be performed. However, if the patient has aged significantly, developed a massive rotator cuff tear in the interim, or if the glenoid bone stock is severely compromised, a Reverse Total Shoulder Arthroplasty (RTSA) becomes the salvage procedure of choice.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Axillary Nerve Injury | < 1% | Direct visualization, stay on bone at 6 o'clock, avoid plunging | Observation, EMG at 3 months, possible nerve exploration/transfer |
| Inadequate Glenoidplasty | 5 - 10% | Pre-op 3D CT templating, meticulous intra-op assessment | Revision arthroscopy vs. Conversion to TSA |
| Excessive Bone Resection | 2 - 5% | Frequent checking of depth, avoid attempting 0° version | May necessitate bone grafting during future TSA/RTSA |
| Recurrent Stiffness | 10 - 15% | Aggressive early PT, adequate intra-op capsular release | Manipulation under anesthesia, arthroscopic lysis of adhesions |
| Progression of OA / Failure | 100% (Long-term) | Proper patient selection (buying time, not curing) | Conversion to Anatomic TSA or Reverse TSA |
| Deep Infection | < 0.5% | Strict sterility, perioperative antibiotics | Arthroscopic I&D, culture-specific IV antibiotics |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following an arthroscopic osteocapsular arthroplasty and glenoidplasty is markedly different from protocols following labral repairs or rotator cuff surgeries. Because the primary goal of the surgery is to restore range of motion through extensive capsular release and bony decompression, the rehabilitation must be immediate, aggressive, and focused on preventing the reformation of scar tissue and capsular contracture. Immobilization is strictly minimized.
Phase I: Immediate Motion Phase (Weeks 0-2)
Patients are placed in a simple clinical sling postoperatively, but this is strictly for comfort and is typically discarded within the first 3 to 7 days. Physical therapy commences on postoperative day one or two. The immediate focus is on aggressive passive range of motion (PROM) and active-assisted range of motion (AAROM) in all planes. The interscalene block placed preoperatively provides a critical window of analgesia allowing the physical therapist to push the shoulder through the newly acquired arc of motion. Patients are instructed to perform pendulum exercises, pulley exercises for forward elevation, and external rotation stretching with a cane multiple times a day. Cryotherapy is utilized extensively to manage the significant postoperative hemarthrosis and inflammation associated with the extensive bony burring.
Phase II: Active Motion and Early Strengthening (Weeks 2-6)
As
