Mastering Shoulder Arthroscopic Approaches: Key Techniques
Introduction & Epidemiology
Shoulder arthroscopy has revolutionized the diagnosis and treatment of a vast array of glenohumeral and periarticular pathologies. Evolving from a purely diagnostic tool in the mid-20th century, it has matured into a sophisticated platform for complex reconstructive procedures, offering reduced morbidity, faster recovery, and improved cosmetic outcomes compared to traditional open approaches. The minimally invasive nature, coupled with advancements in instrumentation, imaging, and surgical techniques, has propelled arthroscopy to the forefront of orthopedic shoulder surgery.
Epidemiologically, shoulder pain is a common musculoskeletal complaint, with a significant burden on healthcare systems. Rotator cuff pathology, glenohumeral instability, and impingement syndromes represent a large proportion of cases, with incidence increasing with age and activity levels. For instance, rotator cuff tears are prevalent in up to 30% of individuals over 60 years old, with arthroscopic repair rates steadily climbing. Similarly, shoulder instability, particularly in young, active populations, frequently necessitates arthroscopic stabilization. The understanding of intricate shoulder anatomy and biomechanics, combined with precise arthroscopic skills, is paramount for optimizing patient outcomes in this expanding surgical domain.
Surgical Anatomy & Biomechanics
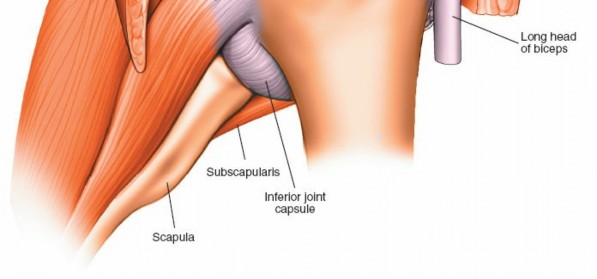
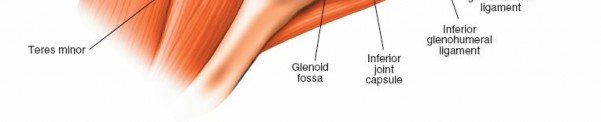
A thorough understanding of shoulder anatomy and biomechanics is indispensable for safe and effective arthroscopic intervention. The shoulder complex comprises four joints: the glenohumeral, acromioclavicular (AC), sternoclavicular, and scapulothoracic articulations. The glenohumeral joint, a ball-and-socket synovial joint, offers the greatest range of motion in the body, a characteristic facilitated by its inherent bony incongruence. Stability is primarily provided by dynamic stabilizers (rotator cuff muscles: supraspinatus, infraspinatus, teres minor, subscapularis) and static stabilizers (glenohumeral ligaments, labrum, joint capsule, negative intra-articular pressure).
Key anatomical structures visualized arthroscopically include:
*
Glenohumeral Joint:
*
Articular Cartilage:
Covering the humeral head and glenoid, susceptible to chondral lesions.
*
Glenoid Labrum:
A fibrocartilaginous rim that deepens the glenoid fossa, enhancing stability. Lesions (e.g., Bankart, SLAP) are common in instability and trauma.
*
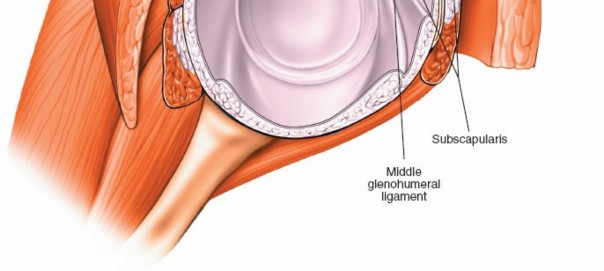
Glenohumeral Ligaments (Superior, Middle, Inferior):
Capsular thickenings vital for static stability, particularly the inferior glenohumeral ligament complex with its anterior and posterior bands.
*
Biceps Tendon (Long Head):
Originates from the superior labrum (supraglenoid tubercle) and traverses the joint. Pathologies include instability, tenosynovitis, and tears.
*
Rotator Cuff Tendons:
The articular surfaces of the supraspinatus, infraspinatus, and subscapularis are visible from within the joint, allowing assessment of partial articular-sided tears.
*
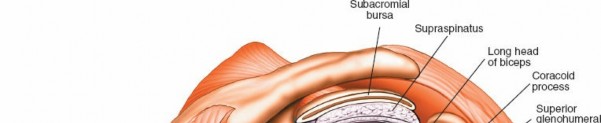
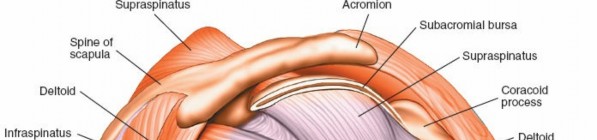
Subacromial Space:
*
Rotator Cuff (Bursal Surface):
The supraspinatus, infraspinatus, and subscapularis tendons. Full-thickness tears and bursal-sided partial tears are observed here.
*
Subacromial Bursa:
A synovial lining that reduces friction between the rotator cuff and the overlying acromion/deltoid. Often inflamed (bursitis) or scarred in impingement syndromes.
*
Acromion:
The undersurface morphology (Type I, II, III) and osteophytes are crucial in subacromial impingement.
*
Coracoacromial Ligament (CAL):
Forms part of the coracoacromial arch.
*
Acromioclavicular (AC) Joint:
The undersurface of the distal clavicle and acromion are visible, allowing assessment of arthritis or osteophyte formation.
Biomechanically, the deltoid and rotator cuff act as a force couple. The rotator cuff depresses and compresses the humeral head into the glenoid, providing a stable fulcrum for the powerful deltoid to elevate the arm. Disruption of this balance, such as with a rotator cuff tear or labral injury, compromises stability and kinematics, leading to pain and dysfunction. Arthroscopic intervention aims to restore this delicate balance.
Indications & Contraindications
The indications for shoulder arthroscopy are broad and continue to expand with technical advancements. Generally, arthroscopic surgery is considered for patients with shoulder pain and dysfunction refractory to adequate non-operative management, where a specific pathology amenable to surgical repair or debridement has been identified.
Indications for Arthroscopic Shoulder Surgery
-
Rotator Cuff Pathology:
- Full-thickness rotator cuff tears (acute or chronic).
- Symptomatic partial-thickness rotator cuff tears (PASTA or bursal-sided).
- Calcific tendinitis refractory to conservative management.
- Subacromial impingement syndrome with bursitis and/or osteophytes.
-
Glenohumeral Instability:
- Anterior, posterior, or multidirectional instability.
- Labral tears (Bankart, SLAP lesions, posterior labral tears).
- Capsular laxity or redundant capsule.
-
Biceps Tendon Pathology:
- Symptomatic biceps tendinopathy or tenosynovitis.
- Partial tears or instability of the long head of biceps.
- SLAP lesions (Type II, III, IV).
-
Articular Cartilage Lesions:
- Localized chondral defects.
- Loose bodies.
-
Adhesive Capsulitis (Frozen Shoulder):
- Diagnostic evaluation and arthroscopic capsular release in recalcitrant cases.
-
Acromioclavicular (AC) Joint Pathology:
- Distal clavicle osteolysis or arthritis requiring arthroscopic distal clavicle excision.
- AC joint instability (less commonly primary arthroscopic repair).
-
Other:
- Synovitis.
- Infection (lavage and debridement).
- Selected cases of glenohumeral osteoarthritis (debridement, microfracture).
- Fracture management (e.g., greater tuberosity fixation, glenoid rim fractures).
Contraindications
Absolute contraindications are rare but include active infection in or around the shoulder joint, severe systemic illness precluding general anesthesia, and inability to tolerate the required patient positioning. Relative contraindications encompass severe glenohumeral osteoarthritis with significant bone loss (often better managed with arthroplasty), grossly unstable shoulders requiring extensive open reconstruction, severe medical comorbidities, and inadequate patient compliance for post-operative rehabilitation.
| Indication Type | Operative Indications (Arthroscopic) | Non-Operative Indications |
|---|---|---|
| Rotator Cuff | Symptomatic full-thickness tear; failed conservative partial-thickness tear; recalcitrant impingement | Asymptomatic tear; acute tear with minimal retraction; failed non-operative full-thickness tear (low demand); mild impingement |
| Instability | Recurrent instability with Bankart/labral tear; significant Hill-Sachs/glenoid bone loss; failed non-operative management | First-time dislocation (especially in older patients); voluntary subluxation; generalized ligamentous laxity |
| Biceps Tendon | Symptomatic SLAP tears (Type II-IV); biceps tendinopathy refractory to conservative care; biceps instability | Asymptomatic SLAP tear (Type I); mild biceps tendinopathy; spontaneous rupture in low-demand patients |
| Cartilage | Symptomatic chondral defects; loose bodies | Asymptomatic chondral lesions; widespread osteoarthritis (consider arthroplasty) |
| Capsulitis | Refractory painful stiffness (after failed prolonged physical therapy, injections) | Early stages, primary treatment with physical therapy, analgesia, steroid injections |
| AC Joint | Distal clavicle osteolysis/arthritis with failed conservative care | Mild AC joint arthritis; asymptomatic osteolysis |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for a successful arthroscopic outcome. This includes a comprehensive review of the patient's history, physical examination, and advanced imaging (X-rays, MRI, CT scan where indicated). MRI is crucial for assessing rotator cuff integrity, labral pathology, and articular cartilage status. CT scans are invaluable for quantifying bone loss in instability cases or complex fractures. Surgical goals, potential complications, and rehabilitation expectations are thoroughly discussed with the patient.
Anesthesia
Most shoulder arthroscopies are performed under general anesthesia, often supplemented with an interscalene brachial plexus block. The block provides excellent post-operative analgesia, reducing opioid requirements and facilitating early rehabilitation.
Patient Positioning
Two primary positions are utilized:
1.
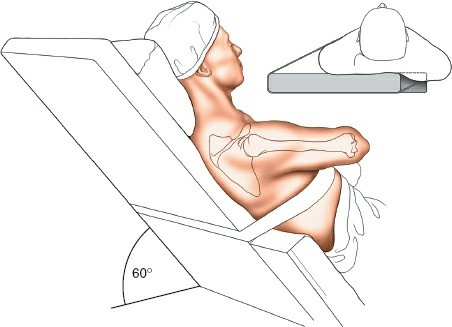
Beach Chair Position:
*
Advantages:
Allows for easy conversion to an open procedure if necessary, facilitates anterior working portals, good ergonomic access to the posterior shoulder, avoids brachial plexus stretch from traction.
*
Setup:
Patient is semi-recumbent, typically at 60-70 degrees of trunk elevation. The head is secured in a headrest (e.g., 'Mayfield' clamp or gel donut) and positioned to allow for adequate neck flexion and rotation away from the operative shoulder, ensuring endotracheal tube security and avoiding cervical strain. The operative arm is draped free and secured in an articulated arm holder, allowing dynamic positioning during the case. The torso is secured to the table to prevent movement. Peripheral pulses are checked.
*

*

*

2.
Lateral Decubitus Position:
*
Advantages:
Provides excellent distraction of the glenohumeral joint with traction, facilitating visualization, particularly in the inferior joint. Good for procedures requiring multiple posterior portals.
*
Setup:
Patient is positioned in the lateral decubitus position on the non-operative side. The torso is secured to the table with beanbags and kidney rests. The operative arm is suspended in traction using a traction tower, typically with 10-15 lbs of weight applied at 30-45 degrees of abduction and 15-20 degrees of forward flexion. Careful padding of all bony prominences (axilla, contralateral ear, peroneal nerve at the fibular head) is critical to prevent nerve injury.
*

*
Regardless of position, the entire shoulder girdle, including the scapula and proximal arm, must be prepped and draped to allow full range of motion intraoperatively.
Detailed Surgical Approach / Technique
General Principles of Arthroscopy
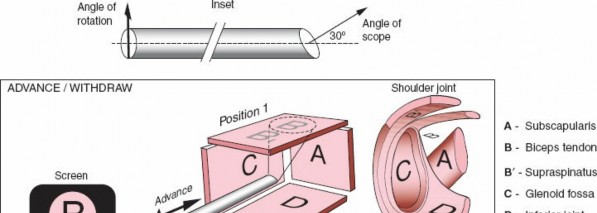
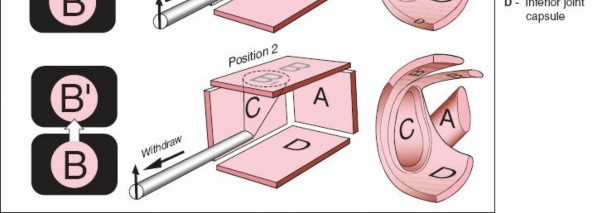
Visualization of anatomic structures in open surgical approaches is straightforward. If a given structure is not visible, it may be exposed by extending the incision, thus expanding the surgical approach. By contrast, visualization of structures in arthroscopic approaches is achieved by using a telescope. The most commonly used arthroscope is angulated 30 degrees at its tip so that the view obtained shows the structures that are 30 degrees from the long axis of the arthroscope and not the structures that are directly in front of the scope. This is the arthroscope described here (Fig. 1-73). Angled scopes are required because the bony structure of the joint allows the arthroscope to be placed only in certain positions. The use of an angled scope allows the surgeon to see “around the corner” and thereby greatly increases the view obtained within any joint.

Keep the following important points in mind during arthroscopic use (Fig. 1-73):
1. Because the scope is angled 30 degrees from its axis, it is not possible to zoom in on an object merely by advancing the scope. The apparent increase in size is due to the camera's fixed focal length and proximity.
2. The area of greatest clarity and definition is at the center of the field of view (Fig. 1-74). Objects at the periphery of the image will be less clearly defined and appear distorted due to the lens physics.
3. You will not be able to visualize those structures directly in front of the arthroscope unless you angle it. This requires rotation of the scope within the portal or subtle manipulation of the scope's angle of entry. (Fig. 1-75).
4. It is possible to change the view by moving the joint while maintaining the scope's position. Dynamic joint positioning can bring various anatomical structures into the field of view.
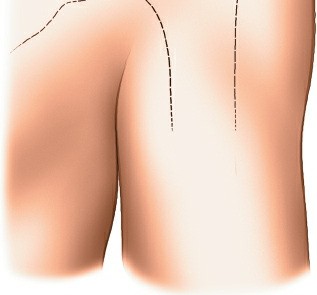
Portal Placement
Accurate and safe portal placement is fundamental. Anatomical landmarks are carefully identified and marked. Infiltration with a local anesthetic containing epinephrine can aid in hemostasis.
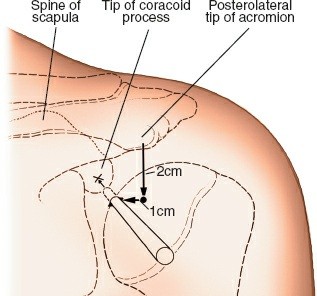
1. Posterior Portal (Standard Diagnostic Portal)
- Location: Approximately 2-3 cm inferior and 1 cm medial to the posterolateral corner of the acromion. This corresponds to the soft spot in the rotator cuff interval.
- Technique: A small skin incision is made. A blunt trocar and cannula are advanced towards the glenoid, aiming anteriorly towards the coracoid process. A palpable "pop" indicates capsular penetration.
- Neurovascular Risk: Axillary nerve (inferior).
-
 -
 -
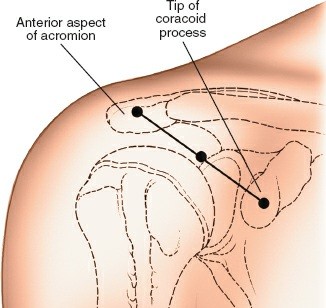
2. Anterior Portals (Working Portals)
Established under direct arthroscopic visualization from the posterior portal.
*
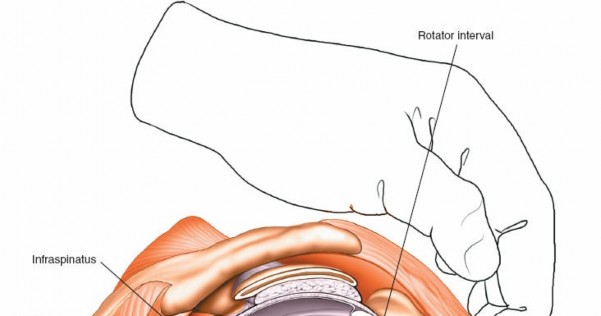
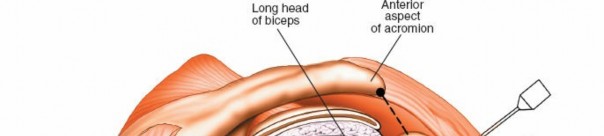
Anterosuperior Portal:
*
Location:
Often in the rotator cuff interval, lateral to the coracoid process.
*
Technique:
An 18-gauge spinal needle is used to localize the ideal entry point. Incision, followed by blunt trocar insertion, ensuring visualization throughout.
*
Neurovascular Risk:
Cephalic vein, musculocutaneous nerve, axillary nerve (distal).
*
*
Anteroinferior Portal:
*
Location:
More inferior than the anterosuperior, typically for inferior labral repair.
*
Technique:
Similar to anterosuperior, guided by spinal needle.
*
Neurovascular Risk:
Axillary nerve. Requires careful consideration, especially in the beach chair position.
*
3. Lateral Portals (Subacromial Working Portals)
Primarily used for subacromial decompression and rotator cuff repair.
*
Location:
Typically 3-4 cm lateral to the acromial border, or directly over the lateral aspect of the acromion.
*
Technique:
Established after shifting the arthroscope to the posterior subacromial portal. A spinal needle confirms placement.
*
Neurovascular Risk:
Axillary nerve (can be within 5 cm of the lateral acromial border).
*

*
4. Accessory Portals
- Anterolateral Portal: Often used for viewing in beach chair.
- Posterolateral Portal: Useful for posterior labral work or specific cuff repairs in lateral decubitus.
- Suprascapular Nerve Portal (Neviaser Portal): For access to the suprascapular notch or spinoglenoid notch.
-

Diagnostic Arthroscopy
A systematic diagnostic arthroscopy of the glenohumeral joint is performed from the posterior portal.
*
Initial Survey:
Assess global synovial health, presence of loose bodies.
*
Biceps Tendon:
Evaluate the long head of the biceps tendon, its sheath, and anchor at the superior labrum. Look for fraying, instability, or SLAP lesions.
*
Superior Labrum:
Assess the SLAP complex and its integrity.

*
Anterior Labrum and Ligaments:
Evaluate the superior, middle, and inferior glenohumeral ligaments, focusing on the anterior band of the IGHL and its attachment to the anterior inferior labrum (Bankart lesion assessment).
*
Inferior Joint:
Assess the axillary pouch and redundant capsule.
*
Posterior Labrum:
Evaluate the posterior labrum for tears, particularly in cases of posterior instability.
*
Glenoid and Humeral Head Articular Cartilage:
Inspect for chondral defects, delamination, or osteochondral lesions (e.g., Hill-Sachs lesion on the humeral head).

*
Rotator Cuff (Articular Surface):
Examine the articular side of the rotator cuff tendons (supraspinatus, infraspinatus, subscapularis) for partial-thickness tears (PASTA lesions).

Following glenohumeral assessment, the arthroscope is typically transitioned into the subacromial space to evaluate the bursal surface of the rotator cuff, the subacromial bursa, and the undersurface of the acromion.
*
Subacromial Bursa:
Evaluate for inflammation, hypertrophy, and fibrosis. Bursectomy is often performed for visualization and decompression.
*
Rotator Cuff (Bursal Surface):
Inspect the bursal side of the rotator cuff for full-thickness tears or bursal-sided partial tears.
*
Acromion and Coracoacromial Ligament:
Assess acromial morphology, osteophytes, and the CAL for impingement.
Specific Surgical Techniques
1. Subacromial Decompression and Rotator Cuff Repair
*
Bursectomy:
Resection of inflamed subacromial bursa using a shaver to expose the rotator cuff and undersurface of the acromion.
*
Acromioplasty:
Resection of anterior and lateral acromial spurs and the undersurface of the acromion using a burr, typically from a lateral portal. This aims to create adequate space for the rotator cuff.
*
Rotator Cuff Repair (RCR):
*
Tear Assessment:
Characterize tear pattern (crescent, L-shaped, U-shaped), size, quality of tissue, and retraction.
*
Mobilization:
Release adhesions and perform careful debridement of torn edges to expose a healthy footprint.
*
Footprint Preparation:
Decortication of the greater tuberosity footprint to create a bleeding bed for tendon-to-bone healing.
*
Anchor Placement:
Suture anchors (singly or doubly loaded) are placed into the bone footprint. Techniques include single-row, double-row, or transosseous equivalent repairs depending on tear pattern, size, and surgeon preference.
*
Suture Management and Knot Tying:
Sutures are passed through the mobilized tendon and secured to anchors, employing various knot-tying techniques (e.g., sliding knots, non-sliding knots).
*
2. Labral Repair for Instability
*
Lesion Assessment:
Identify the type and extent of labral pathology (e.g., Bankart lesion, ALPSA lesion, capsular avulsion).
*
Glenoid Preparation:
Debridement of the glenoid rim to create a bleeding surface for labral reattachment.
*
Anchor Placement:
Suture anchors are strategically placed along the glenoid rim. Typical placement is at 3:00, 4:30, and 6:00 for anterior inferior lesions (right shoulder).
*
Suture Management and Labral Reduction:
Sutures are passed through the torn labral tissue, reducing it back to the glenoid rim and securing it with knots, restoring the bumper function and tensioning the capsule.
3. Biceps Tenodesis/Tenotomy
*
Indications:
Symptomatic biceps tendinopathy, partial tears, instability, or concomitant with SLAP repair in older patients.
*
Tenotomy:
Simple transection of the long head of the biceps tendon from its glenoid origin. Less invasive, quicker, but can lead to "Popeye" deformity.
*
Tenodesis:
Reattachment of the biceps tendon to the humerus. Can be performed entirely arthroscopically (e.g., suprapectoral) or as an arthroscopic-assisted mini-open procedure (e.g., subpectoral). A common technique involves releasing the biceps intra-articularly, retrieving the tendon, preparing it, and fixing it into a drilled hole in the humerus with an interference screw or suture anchor.
4. Arthroscopic Capsular Release for Adhesive Capsulitis
*
Procedure:
A circumferential release of the glenohumeral capsule, often targeting the rotator interval, inferior capsule, and posterior capsule, using a shaver or radiofrequency ablator. Careful control of bleeding and protection of neurovascular structures (especially axillary nerve inferiorly) are crucial. This is typically performed after diagnostic arthroscopy confirms the diagnosis and rules out other significant pathology.
Fluid Management
Maintaining adequate fluid pressure (typically 40-70 mmHg) is critical for joint distension, visualization, and lavage. Infusion pumps are commonly used. Excessive extravasation can lead to complications such as upper extremity compartment syndrome, airway compromise, or neurological deficits. Careful monitoring of inflow/outflow and fluid balance is essential.
Complications & Management
While shoulder arthroscopy is generally safe, a range of complications can occur. Prevention through meticulous technique, thorough anatomical knowledge, and careful patient selection is paramount.
| Complication | Incidence | Salvage Strategies / Management |
|---|---|---|
| Neurovascular Injury | <0.5% (Axillary nerve most common) | Early recognition, nerve exploration, direct repair or grafting, neurolysis. |
| Infection (Septic Arthritis) | 0.1-0.5% | Prompt irrigation and debridement, targeted intravenous antibiotics, repeated debridement if needed. |
| Chondral Injury | 1-5% (iatrogenic during portal creation or instrumentation) | Debridement of unstable fragments; microfracture for full-thickness lesions; OATs for larger defects. |
| Fluid Extravasation/Compartment Syndrome | Rare (e.g., airway compromise) | Cessation of procedure, emergent intubation, fasciotomy (if extremity compartment syndrome). |
| Hardware Complications | 1-2% (anchor pull-out, suture breakage) | Revision surgery, removal of symptomatic hardware, non-operative management for asymptomatic issues. |
| Adhesive Capsulitis (Post-operative) | 5-10% (higher in RCR, diabetes) | Aggressive physical therapy, steroid injections, manipulation under anesthesia, arthroscopic capsular release. |
| Recurrent Instability/Failure of Repair | Varies by procedure (e.g., 5-20% for instability) | Revision surgery, open reconstruction, bone augmentation procedures. |
| DVT/PE | <0.1% | Anticoagulation, inferior vena cava filter in selected cases. |
| CRPS (Complex Regional Pain Syndrome) | Rare | Multidisciplinary pain management, physical therapy, nerve blocks. |
Management Principles:
*
Neurovascular Injuries:
Intraoperative nerve monitoring, meticulous blunt dissection during portal creation, and maintaining awareness of critical zones minimize risk. If suspected, perform immediate exploration.
*
Infection:
Strict aseptic technique, prophylactic antibiotics. Post-operative infection requires immediate surgical lavage and appropriate antibiotic therapy based on culture results.
*
Fluid Extravasation:
Proper fluid management, limiting operative time, and using appropriate pump pressures are critical. Recognize signs of swelling in the neck/chest and manage airway immediately if compromised.
*
Stiffness:
Early, controlled range of motion protocols, particularly after capsular release. Aggressive rehabilitation and, if necessary, secondary arthroscopic capsular release or manipulation under anesthesia.
Post-Operative Rehabilitation Protocols
Rehabilitation after shoulder arthroscopy is critical for restoring function, preventing stiffness, and optimizing long-term outcomes. Protocols are tailored to the specific procedure performed, tear size, tissue quality, and patient factors, but generally follow a phased approach.
General Principles
- Pain Management: Multimodal analgesia including regional blocks, NSAIDs, and acetaminophen.
- Protection of Repair: Initial immobilization with slings for 4-6 weeks for rotator cuff repairs or labral repairs. Passive motion often initiated early, followed by active-assisted and active motion.
- Gradual Progression: Systematic advancement through phases, with specific milestones for each phase.
- Patient Education: Crucial for compliance and understanding limitations.
Phased Rehabilitation Approach (Example for Rotator Cuff Repair)
Phase I: Protection & Early Passive Motion (Weeks 0-6)
- Goals: Protect the repair, reduce pain and inflammation, achieve passive range of motion (PROM).
-
Activities:
- Sling immobilization (removed for exercises and hygiene).
- Pendulum exercises.
- Passive range of motion: external rotation (limited to 0-30 degrees), forward flexion (up to 90-120 degrees), abduction (up to 90 degrees). No active elevation or rotation.
- Scapular stabilization exercises (isometrics, gentle shrugs).
- Precautions: No active elevation, lifting, or supporting body weight with the operative arm. Avoid reaching behind the back or excessive external rotation.
Phase II: Active-Assisted Range of Motion & Gentle Strengthening (Weeks 6-12)
- Goals: Restore full non-painful PROM, initiate active range of motion (AROM), begin light strengthening.
-
Activities:
- Discontinue sling (as tolerated).
- Active-assisted range of motion (AAROM): pulleys, cane exercises.
- Initiate AROM as pain allows.
- Gentle isometric rotator cuff strengthening.
- Scapular strengthening: rows, low-level serratus anterior activation.
- Light resistance exercises for deltoid and periscapular muscles.
- Precautions: Avoid heavy lifting, sudden movements, or forceful pushing/pulling. No overhead lifting beyond what can be comfortably achieved with good form.
Phase III: Moderate Strengthening & Advanced Proprioception (Weeks 12-24)
- Goals: Restore full AROM, progressively increase strength and endurance, improve neuromuscular control.
-
Activities:
- Progressive resistive exercises for rotator cuff and periscapular muscles (bands, light weights).
- Closed kinetic chain exercises.
- Proprioceptive training.
- Introduction of light sport-specific drills for athletes.
- Emphasis on good movement patterns and posture.
- Precautions: Continue to avoid aggressive, high-impact activities. Progress resistance slowly.
Phase IV: Return to Activity (Weeks 24+)
- Goals: Achieve maximal functional strength and endurance, safe return to work, sport, or desired activities.
-
Activities:
- Advanced strengthening and plyometrics.
- Full sport-specific training.
- Gradual return to throwing, overhead activities, and contact sports as appropriate, based on strength, endurance, and surgeon/therapist assessment.
- Criteria for Return to Sport: Full pain-free range of motion, no tenderness, >90% strength compared to contralateral side, satisfactory functional testing.
For other procedures, such as isolated labral repair for instability, the immobilization phase might be shorter (3-4 weeks), with a greater emphasis on restoring stability and preventing recurrent dislocation. For capsular release, early and aggressive range of motion is paramount.
Summary of Key Literature / Guidelines
The landscape of shoulder arthroscopy is continuously shaped by ongoing research and technological advancements. Key literature consistently highlights several themes:
-
Rotator Cuff Repair (RCR): Current evidence supports arthroscopic RCR for symptomatic full-thickness tears, with comparable outcomes to open repair but often with less post-operative pain and improved cosmesis. Meta-analyses demonstrate good to excellent functional outcomes in 80-90% of patients. Factors affecting healing include tear size, tendon retraction, tissue quality, and patient age/comorbidities. Double-row and transosseous equivalent repair constructs have shown biomechanical superiority in some studies, but clinical superiority over single-row repairs remains debated and may be tear-specific.
- Guideline Reference: AAOS Clinical Practice Guidelines for the Management of Rotator Cuff Tears often emphasize shared decision-making and individualized treatment plans.
-
Glenohumeral Instability: Arthroscopic stabilization for traumatic anterior instability (Bankart repair) demonstrates high success rates (80-95%) in preventing recurrent dislocation, particularly in appropriately selected patients (e.g., first-time dislocations, no significant bone loss). For patients with substantial glenoid bone loss (>20-25%) or large Hill-Sachs lesions, arthroscopic bone augmentation procedures (e.g., Remplissage for engaging Hill-Sachs, arthroscopic Latarjet procedure for glenoid bone loss) or open procedures may offer superior stability. The role of capsular plication in multidirectional instability is well-established.
- Guideline Reference: ISAKOS (International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine) and AOSSM (American Orthopaedic Society for Sports Medicine) provide guidelines for instability management.
-
Biceps Pathology & SLAP Lesions: Management of superior labrum anterior-posterior (SLAP) lesions and biceps tendinopathy remains an area of ongoing discussion. For Type II SLAP lesions, repair versus biceps tenodesis/tenotomy depends on patient age, activity level, and associated pathology. Tenodesis often preferred in patients over 40-50, while repair may be considered in younger, high-demand overhead athletes. Evidence suggests similar outcomes for tenodesis versus tenotomy in terms of pain relief, with tenodesis potentially mitigating the "Popeye" deformity.
- Guideline Reference: Consensus statements on SLAP lesions often consider age, activity, and concomitant pathology as critical decision factors.
-
Adhesive Capsulitis: Arthroscopic capsular release is a proven option for patients with recalcitrant adhesive capsulitis who fail extensive non-operative management. Outcomes are generally excellent, particularly in restoring range of motion. Early and aggressive post-operative rehabilitation is crucial.
Continuous professional development and engagement with the latest scientific literature are essential for academic orthopedic surgeons to provide optimal, evidence-based care in the field of shoulder arthroscopy. Mastering these approaches requires not only technical proficiency but also a deep understanding of indications, potential complications, and individualized rehabilitation strategies.
Clinical & Radiographic Imaging