DEFINITION
Posttraumatic conditions of the elbow represent a variety of disorders involving the elbow as a result of previous injury. Included among the posttraumatic conditions are as follows:Posttraumatic arthritisPrimary pathology involves posttraumatic degeneration of the articular surface. Secondary pathologies can include contracture, loose bodies, and heterotopic bone.Nonunion of the distal humerusPresent with different amounts of bone loss and instability through the nonunionOften results from inadequate internal fixation of distal humerus fractures and typically occurs in the supracondylar regionTotal elbow arthroplasty (TEA) is considered when reconstruction of the nonunion is deemed impossible or undesirable.Dysfunctional instability of the elbowSpecial clinical situation where the fulcrum for stable elbow function is lost.15 The forearm is dissociated from the brachium with the forearm displaced medially and contracted proximally (FIG 1). This leads to attenuation of the lateral soft tissues and contracture of the medial soft tissues.Chronic instability (dislocation)Chronic ligamentous instability of the elbow can lead to progressive articular cartilage degeneration and subchondral bone loss, particularly in the elderly, osteopenic patient. FIG 1 • Radiograph demonstrating dissociation of the forearm from the brachium in a patient with an inadequately treated fracture of the distal humerus with resultant nonunion.

ANATOMY

FIG 2 • Photograph of a patient with dysfunctional instability of the elbow. Notice the prominent distal humerus and proximal migration of the forearm medial to the distal humerus. P.948Chronic instability of the elbow can result from a persistently unstable elbow following dislocation with or without associated fracture. The articular surface is compromised by the initial injury or persistent instability.
PATHOGENESIS
The common pathogenesis of all posttraumatic conditions is an injury to the elbow that compromises the integrity of the articular surface with or without nonarticular involvement of the humerus, ulna, or radius.The articular surface can be directly injured by trauma or can degenerate over time as a result of a remote traumatic event.Periarticular trauma and hemorrhage involving the capsule and musculotendinous tissues about the elbow can lead to intra-articular and periarticular fibrosis leading to intrinsic and extrinsic stiffness of the elbow.
PATIENT HISTORY AND PHYSICAL FINDINGS
PATIENT HISTORY
The patient history is directed at gaining information about the initial injury, treatments undertaken, complications of treatment, presenting complaints, and patient expectations.Detailed investigation of the patient's symptoms should include questions regarding the degree of pain, presence of instability or stiffness, and mechanical symptoms of catching or locking.
PHYSICAL EXAMINATION
Inspection of the elbowPresence and location of previous skin incisions or persistent wounds Alignment of the extremity at rest and with attempted motion Prominent hardwareRange of motionActive range of motion (AROM) is assessed and compared to the opposite side. The degree of motion, smoothness of motion, and feel of the end point is established.Passive range of motion (PROM) is then assessed and compared to the active motion arc.Palpation of the elbow should systematically review all of the bony and soft tissue structures of the elbow.Neurovascular examination should carefully assess motor and sensory function of the extremity.The ulnar nerve needs to be carefully assessed. If previously surgically manipulated, its location should be identified if possible.A functional requirement for consideration of TEA is functional elbow flexion (biceps and brachialis muscles). Functional extension (triceps muscle) is less critical than active flexion but should be carefully assessed.
IMAGING AND OTHER DIAGNOSTIC STUDIES
PLAIN X-RAYS
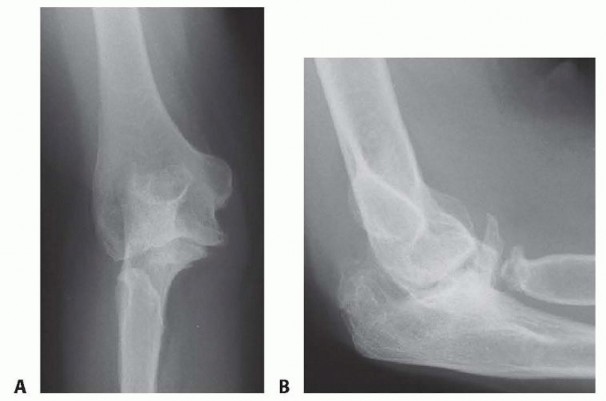
FIG 3 • A,B. AP and lateral radiographs of the elbow in a patient with posttraumatic arthritis of the elbow. Oblique radiographs supplement the AP and lateral images.
ADVANCED IMAGING
Computed tomography (CT) scanCT scans are particularly helpful in assessing the structural integrity of the humerus, radius, and ulna.Identifying the presence of periarticular deformity and the integrity of the articulations are facilitated by CT scan.Three-dimensional reconstructions provide a better understanding of any deformity.Magnetic resonance imaging (MRI)MRI is rarely needed in the assessment of a posttraumatic joint.
DIFFERENTIAL DIAGNOSIS
Nonunion/malunion of the distal humerus Posttraumatic stiffness of the elbow Chronic dislocation of the elbowTraumatic bone loss or surgical excision of bone leading to instability
NONOPERATIVE MANAGEMENT
The success of nonoperative management depends on specific features of the pathology and the motivation and goals of the patient.Activity modification attempts to reduce the forces across the elbow.Overly aggressive attempts to maintain range of motion of the elbow, although commendable, can cause inflammation that is counterproductive to improved motion.External bracing is occasionally used to support an unstable extremity. However, in general, bracing is poorly tolerated and functionally limiting.
SURGICAL MANAGEMENT
Surgical management is directed at addressing the underlying cause of disability, taking into consideration the patient's age, physical requirements, and expectations.P.949
TOTAL ELBOW REPLACEMENT
Patients with posttraumatic conditions of the elbow tend to be younger than other patients undergoing TEA.4,5,6,11,14,15,17In this group of patients, TEA should be considered in patients whoHave failed appropriate nonoperative managementAre not an appropriate candidate for other surgical options Are willing to adopt a more sedentary lifestyleHave no absolute contraindications to the procedure
PREOPERATIVE PLANNING
Implant SelectionImplants are described in terms of their physical linkage (linked, unlinked, or linkable) and on their constraint (constrained, semiconstrained, minimally constrained).Linkage is determined by whether the components are physically joined.Constraint is a more poorly defined quality of an implant. It depends on the geometry of the implant and its interaction with stabilizing soft tissues about the elbow.8Linked (semiconstrained) designsLinked implants have the advantage of being universally applicable to all posttraumatic conditions of the elbow.Unlinked designsThe requirement for the use of unlinked designs in posttraumatic conditions of the elbow is integrity of the collateral ligaments and limited deformity such that normal anatomic relationships can be reestablished.Linkable designsLinkable designs have been developed to take advantage of the features of an unlinked implant while capturing the universal applicability of the linked implants. They can be converted from unlinked to linked either at the time of an initial surgery if stability cannot be conferred or remotely if instability becomes an issue postoperatively.
POSITIONING
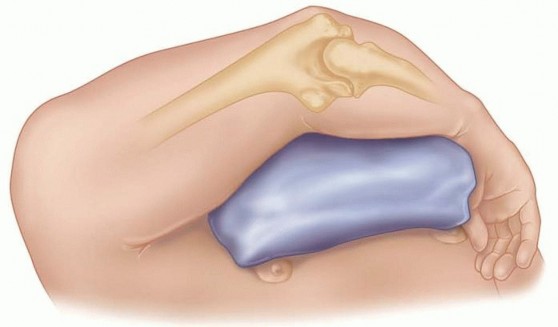
FIG 4 • Patient positioning for TEA with the arm across the body supported on a bolster.
TECHNIQUES
SURGICAL APPROACH
TRICEPS MANAGEMENT


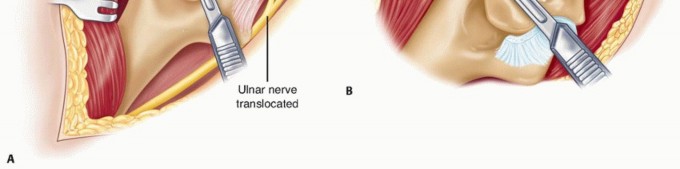
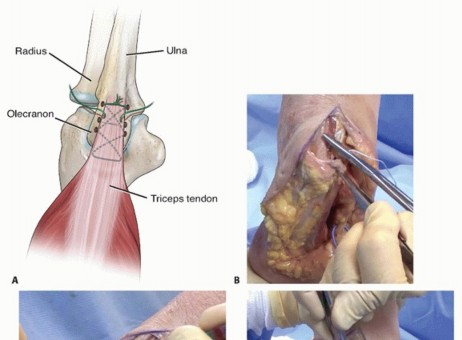
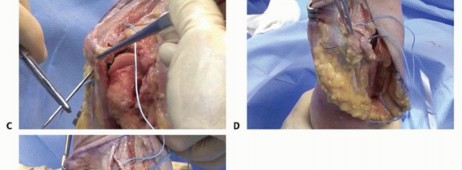
TECH FIG 1 • Bryan-Morrey triceps-reflecting approach. A. The triceps insertion is released in continuity with the anconeus from medial to lateral. B. Further dissection allows the collateral ligaments to be released.
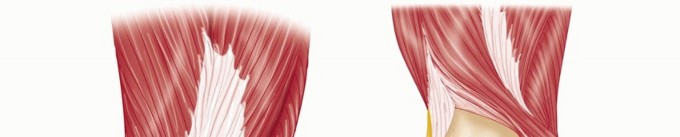



TECH FIG 2 • The osteocutaneous flap approach. A. The triceps is reflected from medial to lateral. B. The triceps insertion is released with a small fleck of the ulnar attachment.
DEEP DISSECTION


TECH FIG 3 • After the LCL and MCL are released, the shoulder is externally rotated and the elbow is hyperflexed to allow the ulna to be separated from the humerus.
Canal Preparation
CANAL PREPARATION
HUMERAL PREPARATION

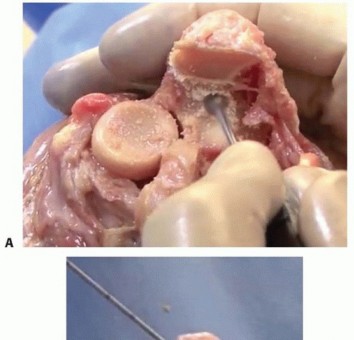
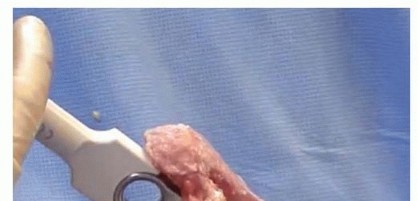
TECH FIG 4 • The central portion of the trochlea is removed in line with the intramedullary canal (A), and the intramedullary canal is opened with a burr (B).
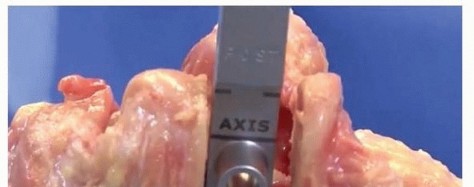

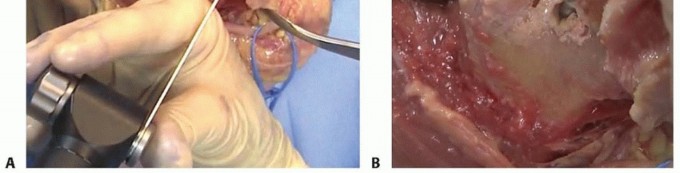
TECH FIG 5 • Humeral rasp is inserted so that the native axis of rotation is coincident with the axis line of the rasp. This guarantees proper depth of insertion of the final humeral component.


TECH FIG 6 • The vertical cutting guide prepares the medial and lateral aspects of the humeral yoke and connects to the trephine score line.


TECH FIG 7 • The trephine stabilizer allows completion of the distal humeral preparation. Proper depth of insertion of this guide may require removal of a small portion of bone from the anterior humerus.
ULNAR PREPARATION

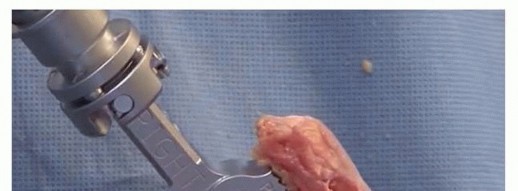
TECH FIG 8 • Ulnar canal preparation begins by (A) opening the intramedullary canal with a burr then


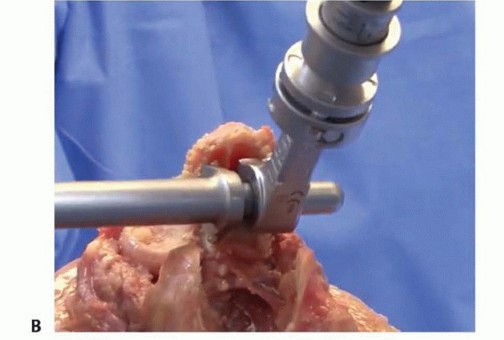
TECH FIG 9 • Proper rotation of the pilot rasp is assured when the back of the rasp is parallel to the flat portion of the dorsal aspect of the olecranon. Sequentially rasp the canal to prepare the proximal ulnar canal. The ulnar canal is sequentially rasped until the eye of the final rasp sits centrally within the native greater sigmoid notch (TECH FIG 10).With the final rasp in place, the ulnar planer is engaged into the medial and lateral aspects of the eye of the rasp to clear bone for the polyethylene ulnar bushing (TECH FIG 11).
TRIAL REDUCTION

TECH FIG 10 • The final rasp is inserted until the eye sits centrally within the native greater sigmoid notch.


TECH FIG 11 • The medial (A) and lateral (B) walls of the ulna are prepared with the ulnar rasp which allows proper seating of the ulnar bushings.
CEMENTING THE IMPLANT


TECH FIG 12 • The humeral and ulnar trial implants are inserted and articulated.

TECH FIG 13 • The ulnar component is inserted so that the ulnar eye sits centered in the greater sigmoid notch.


TECH FIG 14 • The humeral component is inserted into the prepared canal. As the component is inserted, a bone graft is placed behind the anterior flange and the anterior humeral cortex.


TECH FIG 15 • Once the ulnar component is inserted and the cement has hardened, the ulnar bushings are assembled in situ.
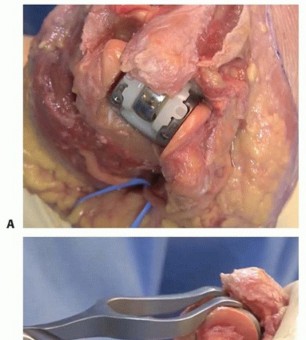
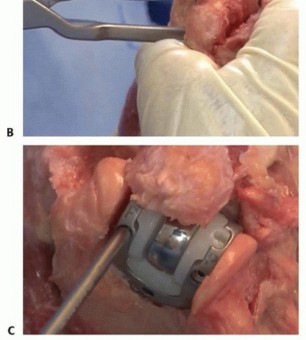
TECH FIG 16 • The ulnar bushings are aligned in the yoke of the humeral component (A) and fully seated with the bushing compression tool (B). Set screws are inserted and tightened with a torque wrench to secure the articulation (C).

TECH FIG 17 • A. The triceps is repaired using cruciate and transverse drill holes. B. The triceps is overreduced and the repair is initiated by passing a suture through the distal medial to proximal lateral cruciate drill hole. C. A series of locking stitches are placed across the triceps, and the cruciate repair is completed by passing the stitch from proximal medial to distal lateral. D. The transverse repair is started by passing the suture from medial to lateral, capturing the triceps. E. Sequential locking sutures are placed across the posterior triceps, sealing it to the ulna. Start suture distally on the medial side of the ulna and direct the needle laterally through the drill hole to capture the lateral triceps tendon with a locking stitch. The suture is brought to the midline of the triceps and a second locking stitch is placed slightly more proximal and in the triceps tendon's midline. The third locking stitch aligns with the medial tunnel in the olecranon,P.956and the suture is drawn through the tunnel emerging on the lateral aspect of the reflected mechanism. Itis brought through the sleeve of tissue from lateral to medial.The transverse repair starts by passing the suture medial to lateral through the olecranon. After piercing the lateral sleeve of tissue, it is brought to the midportion of the triceps tendon, and a locking stitch is placed slightly proximal to the attachment after which it again pierces the medial aspect of the margin of the triceps.The sutures are tied with the elbow in approximately 45 degrees of flexion. The FCU fascia and anconeus are then repaired to surrounding tissue.1. Wound ClosureThe ulnar nerve is transposed into a subcutaneous pocket and held anteriorly with a fascial sling. A subcutaneous drain is place laterally.A layered wound closure is performed.The arm is immobilized in extension with an anterior splint until the drain is removed on the second postoperative day.Indications1. TEA is considered in carefully selected patients where other nonoperative andoperative measures have been exhausted.Goals oftreatment1. The goal of treatment is a pain-free, functional arc of motion.TEA1. Ulnar nerve transposition in all cases2. Triceps-reflecting approach, especially when the joint is very stiff3. Release both the MCL and LCL.4. Release the flexor-pronator and common extensor, particularly if there is significant preoperative deformity.
PEARLS AND PITFALLS
POSTOPERATIVE CARE
The elbow is immobilized in full extension in a well-padded anterior splint.The arm is elevated on pillows or suspended from an intravenous (IV) pole to reduce swelling. The splint is removed 24 to 48 hours after surgery.Gentle AROM is begun in flexion, pronation, and supination. Active extension is avoided for 6 weeks to protect the triceps repair. However, gravity-assisted extension or passive extension is permitted.In general, formal physical therapy is rarely required to regain range of motion. However, formal physical therapy may be beneficial in those patients that struggle to regain their range of motion. The general timeline of therapy is as follows:Phase I (0 to 6 weeks): Protect the soft tissue and begin protected active-assistive range of motion.Phase II (6 to 12 weeks): Continue to improve range of motion. Begin strengthening exercises and encourage functional use of the arm.Phase III (12 to 16 weeks): Return to normal functional activities within the restrictions for TEA. Postoperative stiffness may be helped with splinting. Static splinting is preferred over dynamic splinting. RestrictionsLifetime limitations of the operated extremity include 5-pound repetitive lifting and 10-pound single-event restriction.
OUTCOMES
Patients undergoing TEA for posttraumatic conditions of the elbow tend to be younger, higher demand. TEA for posttraumatic conditions of the elbow is associated with improved clinical outcomes2,3,4,9,10,13,15,16,17Higher complication rate is noted for posttraumatic conditions compared to other indications for TEA.18Mechanical complications such as component fracture and increased polyethylene bushing wear are more common.Causes of increased complications include the following: Multiple previous surgeriesDeformity of the elbow requiring realignment of the extremity through the implant
COMPLICATIONS
TEA for traumatic conditions is associated with a high complication rate. Major complications include the following:Infection7,20Current reports indicate an infection rate of 2% to 5% for primary TEA.Higher infection rates are noted with posttraumatic arthritis and a history of prior surgery.LooseningTriceps insufficiency Underrecognized problemP.957Neurologic injuryIncidence of transient ulnar neuropathy is as high as 26% and permanent nerve injury is up to 10%.Wound complications Associated with prior surgeryAvoid wound complications by the following:Manage wound by immobilizing in extension postoperatively. Use of a subcutaneous drain to avoid hematoma formationA significant postoperative hematoma should be evacuated.Periprosthetic fractureCan occur intraoperatively or postoperatively Incidence ranges from 1% to 23%.
REFERENCES
- Celli A, Arash A, Adams RA, et al. Triceps insufficiency following total elbow arthroplasty. J Bone Joint Surg Am 2005;87(9):1957-1964.
- Cil A, Veillette CJ, Sanchez-Sotelo J, et al. Linked elbow replacement: a salvage procedure for distal humeral nonunion. J Bone Joint Surg Am 2008;90(9):1939-1950.
- Espiga X, Antuna SA, Ferreres A. Linked total elbow arthroplasty as treatment of distal humerus nonunions in patients older than 70 years. Acta Orthop Belg 2011;77(3):304-310.
- Figgie HE III, Inglis AE, Ranawat CS, et al. Results of total elbow arthroplasty as a salvage procedure for failed elbow reconstructive operations. Clin Orthop Relat Res 1987;(219):185-193.
- Figgie MP, Inglis AE, Mow CS, et al. Salvage of non-union of supracondylar fracture of the humerus by total elbow arthroplasty. J Bone Joint Surg Am 1989;71(7):1058-1065.
- Inglis AE, Inglis AE Jr, Figgie MM, et al. Total elbow arthroplasty for flail and unstable elbows. J Shoulder Elbow Surg 1997;6(1):29-36.
- Jeon IH, Morrey BF, Anakwenze OA, et al. Incidence and implications of early postoperative wound complications after total elbow arthroplasty. J Shoulder Elbow Surg 2011;20(6):857-865.
- Kamineni S, O'Driscoll SW, Urban M, et al. Intrinsic constraint of unlinked total elbow replacements—the ulnotrochlear joint. J Bone Joint Surg Am 2005;87(9):2019-2027.
- Kodde IF, van Riet RP, Eygendaal D. Semiconstrained total elbow arthroplasty for posttraumatic arthritis or deformities of the elbow: a prospective study. J Hand Surg Am 2013;38(7):1377-1382.
- LaPorte DM, Murphy MS, Moore JR. Distal humerus nonunion after failed internal fixation: reconstruction with total elbow arthroplasty. Am J Orthop 2008;37(10):531-534.
- Moro JK, King GJ. Total elbow arthroplasty in the treatment of posttraumatic conditions of the elbow. Clin Orthop Relat Res 2000;(370):102-114.
- Morrey BF. Surgical exposures of the elbow. In: Morrey BF, Sanchez-Sotelo J, eds. The Elbow and Its Disorders, ed 4. Philadelphia: Saunders Elsevier, 2009:115-142.
- Morrey BF, Adams RA, Bryan RS. Total replacement for post-traumatic arthritis of the elbow. J Bone Joint Surg Br 1991;73(4):607-612.
- Morrey BF, Schneeberger AG. Total elbow arthroplasty for posttraumatic arthrosis. Instr Course Lect 2009;58:495-504.
- Ramsey ML, Adams RA, Morrey BF. Instability of the elbow treated with semiconstrained total elbow arthroplasty. J Bone Joint Surg Am 1999;81(1):38-47.
- Sanchez-Sotelo J, Morrey BF. Linked elbow replacement: a salvage procedure for distal humeral nonunion. Surgical technique. J Bone Joint Surg Am 2009;91(suppl 2):200-212.
- Schneeberger AG, Adams R, Morrey BF. Semiconstrained total elbow replacement for the treatment of post-traumatic osteoarthrosis. J Bone Joint Surg Am 1997;79(8):1211-1222.
- Throckmorton T, Zarkadas P, Sanchez-Sotelo J, et al. Failure patterns after linked semiconstrained total elbow arthroplasty for posttraumatic arthritis. J Bone Joint Surg Am 2010;92(6):1432-1441.
- Wolfe SW, Ranawat CS. The osteo-anconeus flap. An approach for total elbow arthroplasty. J Bone Joint Surg Am 1990;72(5):684-688.
- Yamaguchi K, Adams RA, Morrey BF. Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80(4):481-491.
