External Fixation Pelvis-Femur-Tibia: Expert Approaches
Introduction & Epidemiology
External fixation remains a critical tool in the armamentarium of the orthopedic trauma surgeon, serving as a primary modality for damage control orthopedics (DCO) in polytraumatized patients and, in selected cases, as a definitive stabilization method. This approach offers rapid, minimally invasive stabilization of unstable fractures, control of hemorrhage, and facilitation of soft tissue management, particularly in the pelvis, femur, and tibia.
High-energy trauma, often involving motor vehicle accidents, falls from height, or industrial incidents, frequently results in complex injuries to these anatomical regions. Pelvic ring injuries, with an incidence ranging from 2% to 10% in blunt trauma, are associated with significant morbidity and mortality, primarily due to hemorrhage. Early stabilization with external fixation can reduce pelvic volume, tamponade venous bleeding, and contribute to hemodynamic stability. Femoral and tibial fractures, particularly those that are open, highly comminuted, or associated with severe soft tissue compromise or vascular injury, often necessitate external fixation as a temporary measure. The principles of DCO prioritize physiological stabilization over immediate definitive osteosynthesis in critically ill patients, thereby reducing the "second hit" phenomenon associated with prolonged early definitive surgery. External fixation allows for staged reconstruction, providing time for resuscitation, soft tissue recovery, and thorough pre-operative planning for subsequent definitive procedures.
Surgical Anatomy & Biomechanics
Pelvis
The pelvic ring is a complex osteoligamentous structure designed for weight bearing and force transmission. It comprises the two innominate bones (ilium, ischium, pubis) articulating anteriorly at the pubic symphysis and posteriorly with the sacrum at the sacroiliac (SI) joints. Stability is conferred by strong ligamentous complexes, including the anterior and posterior SI ligaments, sacrotuberous, and sacrospinous ligaments. Disruption of these structures, particularly the posterior ligamentous complex, leads to instability.
External fixation constructs for the pelvis primarily address anterior ring instability or provide initial stabilization for combined anterior and posterior injuries.
*
Iliac Crest Pins:
These pins are placed into the iliac crest, typically immediately posterior to the anterior superior iliac spine (ASIS). The iliac crest provides a broad cancellous corridor between its inner and outer tables. Biomechanically, this construct reduces external rotation and vertical shear forces of the anterior pelvis, effectively closing the "open book" deformity. However, their position relatively superior to the center of rotation of the hemipelvis may limit their ability to fully control rotational forces and can generate cantilever bending moments.
*
Anterior Inferior Iliac Spine (AIIS) Pins:
Pins placed into the AIIS and directed towards the supra-acetabular region offer a more robust anchor point. This technique provides a deeper purchase within denser cortical bone and a more direct force vector for anterior ring compression. The biomechanical advantage lies in a more rigid construct that better controls rotation and translation, given its closer proximity to the center of rotation of the hemipelvis.
Neurovascular structures at risk during pelvic external fixation include:
*
Lateral Femoral Cutaneous Nerve (LFCN):
Courses over or pierces the inguinal ligament near the ASIS. Highly vulnerable during iliac crest pin insertion.
*
Femoral Neurovascular Bundle:
Located medial to the AIIS. At risk during AIIS pin placement, especially if directed too medially or deeply.
*
Superior Gluteal Vessels/Nerve:
Located near the greater sciatic notch, at risk with deep posterior screw placement, less relevant for anterior external fixation.
Femur
The femur is the longest and strongest bone in the body, critical for weight bearing and locomotion. It is highly constrained by powerful musculature.
*
Proximal Femur:
Comprises the femoral head, neck, greater, and lesser trochanters. Fractures here often involve substantial muscle forces (glutei, iliopsoas).
*
Femoral Diaphysis:
Characterized by thick cortical bone, providing excellent purchase for pins. Surrounded by quadriceps, hamstrings, and adductor muscles.
*
Distal Femur:
Metaphyseal and epiphyseal regions, forming the knee joint. This area is relatively cancellous, especially within the condyles.
Biomechanically, femoral external fixation aims to neutralize bending, rotational, and axial forces. Pin placement strategy involves selecting robust cortical bone for purchase, minimizing muscle impingement, and avoiding neurovascular structures. Safe zones for pin placement:
*
Proximal Femur:
Lateral aspect of the greater trochanter or subtrochanteric region. Anterior placement can be considered but must avoid the femoral neurovascular bundle.
*
Distal Femur:
Anterolateral or lateral supracondylar region, proximal to the joint line. Avoidance of the popliteal neurovascular bundle posteriorly.
External fixator constructs for the femur can be monolateral or biplanar, often bridging the knee joint in complex cases or non-bridging for diaphyseal fractures.
Tibia
The tibia, particularly its anterior aspect, is subcutaneous, making it prone to open fractures and soft tissue compromise.
*
Proximal Tibia:
Metaphyseal region (tibial plateau), cancellous bone.
*
Tibial Diaphysis:
Thick anterior and medial cortical bone, less robust posteriorly and laterally.
*
Distal Tibia:
Metaphyseal region and malleoli.
Biomechanically, tibial external fixation relies on strong cortical purchase. The goal is to provide stability to allow soft tissue healing and definitive planning.
*
Safe Zones for Pin Placement:
*
Proximal Tibia:
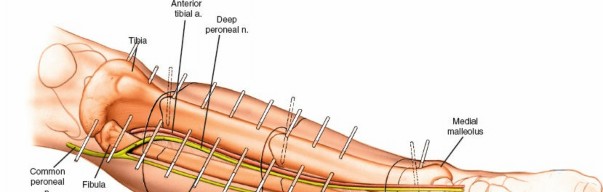
Anteromedial aspect of the tibial metaphysis, approximately 15-20 mm distal to the joint line. Care must be taken to avoid the pes anserinus tendons and the common peroneal nerve laterally as it wraps around the fibular neck.
*
Distal Tibia:
Medial aspect, approximately 15-20 mm proximal to the ankle joint. Avoidance of the saphenous nerve and vein anteromedially.
*
Fibula:
Pins can be placed into the fibula for increased stability, particularly in ankle-spanning frames or bicortical constructs for diaphyseal fractures.
Constructs can range from simple monolateral frames for diaphyseal injuries to more complex biplanar or circular frames (e.g., Ilizarov, Taylor Spatial Frame) for periarticular fractures, segmental defects, or limb lengthening. The relatively thin soft tissue envelope anteriorly and medially requires meticulous pin site care to prevent infection.
Indications & Contraindications
External fixation is primarily a tool for temporary stabilization in polytrauma settings (damage control orthopedics) but also has definitive applications.
Indications
-
Damage Control Orthopedics (DCO):
- Pelvic Ring Injuries: Hemodynamically unstable pelvic fractures (e.g., Young-Burgess APC II/III, vertical shear) to reduce pelvic volume and tamponade hemorrhage.
- Open Fractures: Gustilo-Anderson Type II and III open fractures of the femur and tibia, particularly those with significant contamination or soft tissue loss, to allow debridement and delayed wound closure.
- Polytrauma: Fractures in physiologically unstable patients (e.g., severe head injury, chest trauma, abdominal trauma) who cannot tolerate prolonged definitive surgery.
- Vascular Injury: Fractures associated with major vascular injury requiring repair, allowing skeletal stabilization prior to or concurrent with vascular reconstruction.
- Severe Soft Tissue Swelling/Injury: Compartment syndrome, extensive degloving injuries, or crush injuries where definitive internal fixation would exacerbate tissue damage or increase infection risk.
- Burns: Fractures in burned extremities where internal fixation is complicated by burn wounds.
- Infected Nonunions/Osteomyelitis: As part of a staged approach to débridement and skeletal stabilization.
-
Definitive Fixation:
- Highly comminuted periarticular fractures (e.g., tibial plateau, pilon fractures) with severe soft tissue compromise.
- Segmental bone loss requiring bone transport or limb lengthening.
- Infected nonunions after débridement.
- Fractures in patients with severe comorbidities precluding internal fixation.
Contraindications
-
Absolute Contraindications:
- Patient instability prohibiting any surgical intervention, though external fixation is often performed in resuscitation bay as part of ATLS.
- Severe osteopenia preventing adequate pin purchase.
- Stable fractures amenable to immediate, less invasive definitive treatment (e.g., closed reduction and casting for select tibial shaft fractures).
-
Relative Contraindications:
- Extensive soft tissue scarring or previous surgery compromising safe pin placement.
- Active infection at a planned pin site, though external fixation is often used in the setting of infection at the fracture site itself.
| Indication Type | Operative Indications | Non-Operative Indications |
|---|---|---|
| Pelvis | Hemodynamically unstable pelvic ring injuries (DCO) | Stable pelvic fractures (e.g., APC I, isolated rami) |
| Open pelvic fractures | ||
| Severe pubic symphysis diastasis | ||
| Femur | Open femoral fractures (Gustilo Type II/III) (DCO) | Select stable, nondisplaced femoral shaft fractures (rare) |
| Polytrauma patients with femoral fractures (DCO) | ||
| Femoral fractures with vascular injury (DCO) | ||
| Severe soft tissue compromise around fracture | ||
| Tibia | Open tibial fractures (Gustilo Type II/III) (DCO) | Select stable, closed tibial shaft fractures |
| Polytrauma patients with tibial fractures (DCO) | ||
| Tibial fractures with vascular injury or compartment syndrome | ||
| Highly comminuted periarticular fractures with severe soft tissue compromise (definitive or DCO) | ||
| Bone loss requiring transport / lengthening (definitive) | ||
| Infected nonunions / osteomyelitis (definitive) |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential to minimize surgical time, optimize pin placement, and ensure construct stability.
Pelvis
- Imaging: Initial trauma radiographs (AP pelvis, inlet, outlet views) are crucial. A computed tomography (CT) scan of the pelvis with 3D reconstructions provides detailed anatomical assessment of fracture patterns, ligamentous disruptions, and potential pin corridors.
- Resuscitation: Adherence to Advanced Trauma Life Support (ATLS) protocols is paramount. Patients requiring pelvic external fixation are often hemodynamically unstable, necessitating aggressive fluid resuscitation, blood product transfusion, and potentially vasopressors.
- Positioning: The patient is placed supine on a radiolucent operating table or trauma bay stretcher. The abdomen should be accessible for potential trauma surgery and the lower extremities positioned to allow C-arm fluoroscopy access for both AP and lateral views. Ensure adequate padding to prevent pressure injuries.
- C-arm Setup: The C-arm should be positioned to obtain high-quality fluoroscopic images of the entire anterior pelvis, facilitating accurate ASIS/AIIS identification and pin trajectory assessment.
- Instrumentation: Prepare an external fixator tray with various pin lengths, diameters (typically 5 or 6 mm Schanz screws), clamps, and carbon fiber rods. A sterile drill, drill guide, and pin wrenches are also required.
Femur
- Imaging: AP and lateral radiographs of the femur, including the hip and knee joints. CT scans are invaluable for complex periarticular fractures (e.g., supracondylar femur) to plan pin placement.
- Positioning: The patient is typically positioned supine on a radiolucent table. Traction can be applied if necessary to achieve length and alignment. For distal femoral fractures, the knee may need to be slightly flexed for optimal visualization. The entire limb must be accessible for C-arm imaging. Lateral positioning may be an option for certain proximal femur fracture patterns.
- C-arm Setup: Ensure full AP and lateral views of the fracture site and pin insertion points can be obtained without repositioning the patient.
- Instrumentation: A standard external fixator set with appropriate length and diameter Schanz pins (e.g., 5 or 6 mm), universal clamps, and rods. A sterile drill, drill guide, and wrenches are essential.
Tibia
- Imaging: AP and lateral radiographs of the tibia, including the knee and ankle joints. CT scans are critical for periarticular fractures (e.g., tibial plateau, pilon) to delineate fracture morphology and guide pin placement.
- Positioning: The patient is positioned supine on a radiolucent table. The entire lower leg and foot must be draped sterilely and allow for manipulation to achieve reduction. The knee can be slightly flexed or extended depending on the fracture location and planned frame.
- C-arm Setup: Ensure full AP and lateral views of the fracture site and planned pin insertion points are obtainable. Oblique views may be necessary for complex periarticular fractures.
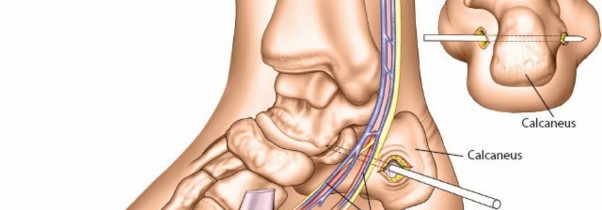
- Instrumentation: External fixator set with appropriate pins (e.g., 4 or 5 mm Schanz screws), clamps, and carbon fiber rods. Sterile drill, drill guides, and wrenches are required. For bridging ankle frames, foot plates or additional pins in the calcaneus/metatarsals may be needed.
General Pre-operative Considerations
- Prophylactic Antibiotics: Administer intravenous broad-spectrum antibiotics, especially for open fractures.
- DVT Prophylaxis: Initiate DVT prophylaxis as per institutional guidelines.
- Sterile Draping: Prepare a wide sterile field to allow for manipulation and C-arm access.
Detailed Surgical Approach / Technique
Pelvis
The primary goal of pelvic external fixation is rapid stabilization of the anterior pelvic ring to reduce intrapelvic volume, provide hemodynamic stability, and reduce pain.
Iliac Crest External Fixation
This technique is relatively straightforward and rapid, making it suitable for unstable patients in the trauma bay.
1.
Patient Positioning:
Supine on a radiolucent table, allowing fluoroscopy access.
2.
Landmarking & Incision:
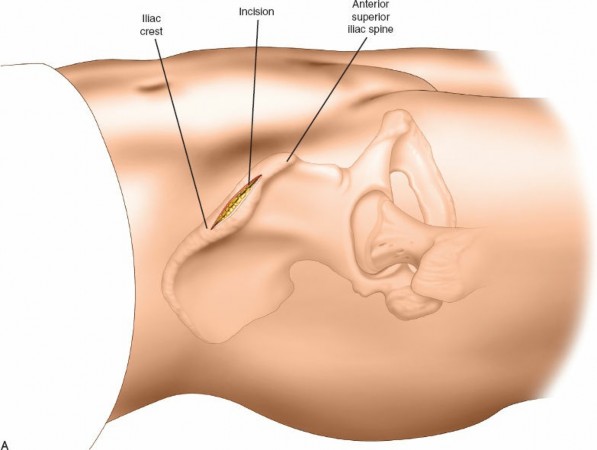
Palpate the anterior superior iliac spine (ASIS). Make a small (2-3 cm) longitudinal incision immediately posterior to the ASIS on the subcutaneous surface of the iliac crest. This posterior placement mitigates direct irritation of the lateral femoral cutaneous nerve (LFCN), which typically crosses anterior to or directly over the ASIS. Perform this bilaterally.

3.
Dissection:
Carefully incise the skin and subcutaneous tissue. Bluntly dissect down to the outer table of the iliac crest using scissors or a small blunt spreader. Ensure direct visualization of the bone.
4.
Pin Placement Site:
Identify a suitable pin insertion site approximately 1.5-2 cm posterior to the ASIS along the iliac crest.
5.
Pilot Hole & Pin Insertion:
Using a drill guide, drill through the outer cortex only, perpendicular to the outer table. Confirm trajectory with fluoroscopy.
The seed content explicitly states: "Only drill the outer cortex and introduce the pins by hand, allowing them to slide between the two tables of the iliac wing." This "bithalamic" approach guides the pin within the cancellous bone between the inner and outer tables of the ilium.
To aid in correct pin placement, especially when the bone is displaced: "Introducing long needles on either side of the iliac wing, keeping them in contact with the bone, provides a useful guide to correct pin placement."

Insert a 5 or 6 mm Schanz screw by hand, aiming posteriorly and slightly medially to maximize bone purchase. Fluoroscopy (inlet and outlet views) is essential to confirm the pin trajectory and ensure it does not violate the inner table, gluteal musculature, or hip joint. Advance the pin approximately 6-8 cm. A second pin can be placed parallel and approximately 2 cm posterior to the first, following the same technique.
Repeat on the contralateral side.
6.
Frame Assembly:
Connect the four pins (two per side) using carbon fiber rods and universal clamps. Create a sturdy A-frame or rectangular frame anteriorly. Compress the frame to close the "open book" deformity and reduce pelvic volume. Fluoroscopic images (AP, inlet, outlet) confirm reduction.
 (This image seems to show a pelvic frame, possibly with AIIS pins, but can illustrate the general concept of frame assembly as the final image for the pelvis section).
(This image seems to show a pelvic frame, possibly with AIIS pins, but can illustrate the general concept of frame assembly as the final image for the pelvis section).
Anterior Inferior Iliac Spine (AIIS) External Fixation
This technique offers increased stability compared to iliac crest fixation but is more technically demanding and carries a higher risk of neurovascular injury if not performed meticulously.
1.
Patient Positioning & Landmarking:
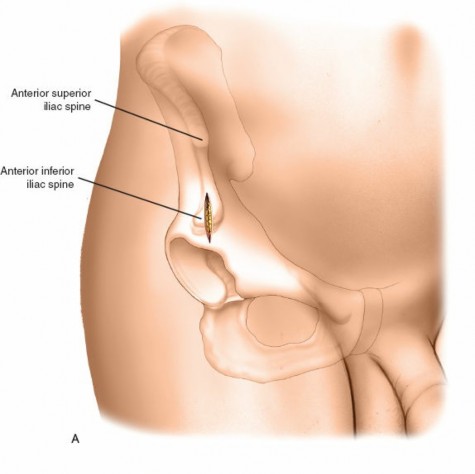
Supine. Identify the ASIS, and then the AIIS approximately 2-3 cm inferior and slightly medial to the ASIS. This landmark can be challenging to palpate, especially in obese patients, and thus necessitates fluoroscopic guidance.
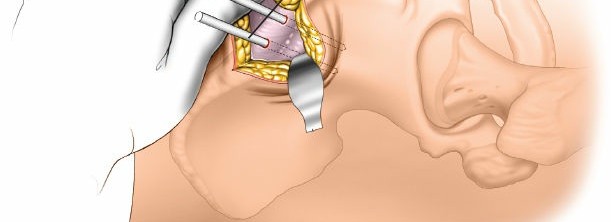
2.
Incision:
A larger (4-6 cm) longitudinal incision is often required, starting at the ASIS and extending distally and slightly medially, paralleling the sartorius muscle.
3.
Dissection:
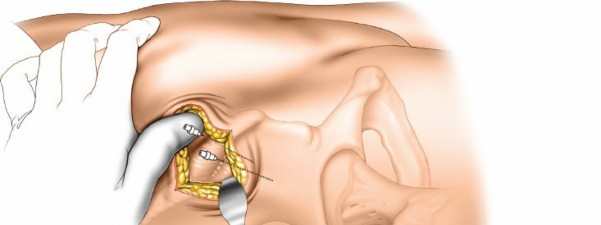
Carefully dissect through subcutaneous tissue. The sartorius muscle originates from the ASIS and AIIS. Retract the sartorius muscle laterally to expose the AIIS. Exercise extreme caution to protect the femoral neurovascular bundle, which lies medial to the AIIS. Palpate the femoral artery throughout the dissection to ensure it is not encroached upon.
 (This image can represent AIIS landmarking/dissection)
(This image can represent AIIS landmarking/dissection)
4.
Pin Placement:
* Place a small Hohmann retractor around the AIIS to facilitate exposure and provide a tactile guide.
* Using fluoroscopy (obturator oblique view and AP view), identify the optimal trajectory into the dense bone of the AIIS, aiming for the supra-acetabular corridor. The trajectory should be directed superiorly, posteriorly, and slightly laterally, avoiding the hip joint.
* Insert a 5 or 6 mm Schanz screw, typically under direct visualization and continuous fluoroscopic monitoring. Bicortical purchase is desirable for maximal stability.
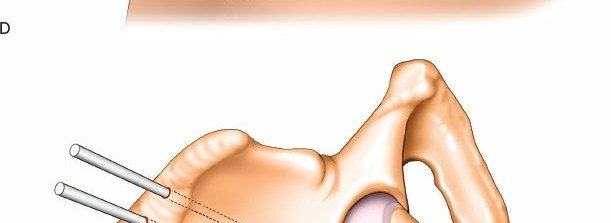 (This image can represent AIIS pin insertion).
(This image can represent AIIS pin insertion).
Repeat on the contralateral side.
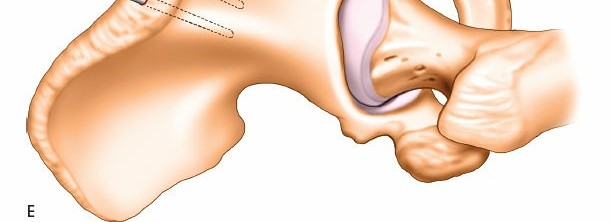
5.
Frame Assembly:
Connect the two AIIS pins with a carbon fiber rod and clamps, creating a robust anterior pelvic frame. Compression can be applied to achieve reduction.
Femur
Femoral external fixation is primarily a DCO technique, often bridging the knee or hip joint depending on the fracture location.
- Patient Positioning: Supine on a radiolucent table, with care to allow full C-arm access to the hip, femur, and knee. Traction may be applied to achieve length.
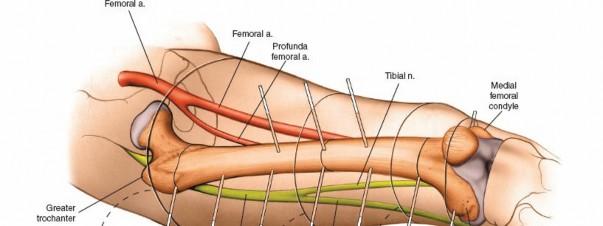
-
Landmarking & Incision:
- Proximal Femur: For diaphyseal fractures, proximal pins are usually placed laterally in the subtrochanteric region, approximately 10-15 cm distal to the greater trochanter. Incision should be small (1-2 cm) and longitudinal.
- Distal Femur: Distal pins are placed anterolaterally or laterally in the supracondylar region, 10-15 cm proximal to the knee joint. The incision is similar.
- Identify safe zones for pin placement to avoid major neurovascular structures (femoral artery/nerve medially and anteriorly in the proximal thigh; popliteal artery/nerve posteriorly in the distal thigh).
- Dissection: Incise skin and subcutaneous tissue. Blunt dissection to bone. Use careful palpation and fluoroscopy to ensure pin trajectory avoids nerves and vessels.
-
Pin Placement:
- Using a drill guide, drill bicortically. Preferred pin size is 5 or 6 mm Schanz screws.
- Insert at least two pins proximally and two pins distally, ensuring sufficient distance from the fracture site (typically at least 5-7 cm from the fracture ends) to allow for subsequent definitive fixation. Spread pins widely within each fragment for optimal stability.
-
Confirm pin placement with fluoroscopy in AP and lateral views. Pins should be parallel within each fragment and perpendicular to the bone's long axis if possible.
 (Example of femoral pin placement)
(Example of femoral pin placement)
-
Frame Assembly:
- Monolateral Frame: Connect the proximal and distal pins with carbon fiber rods and universal clamps. Apply gentle distraction or compression as needed to achieve appropriate length, alignment, and rotation.
-
Bridging vs. Non-bridging:
For simple diaphyseal fractures, a non-bridging frame can be constructed. For complex periarticular fractures (e.g., supracondylar), the frame may bridge the knee joint, immobilizing it in a functional position (e.g., 20-30 degrees of flexion).
 (Example of a femoral external fixator frame)
(Example of a femoral external fixator frame)
Tibia
Tibial external fixation is common for open fractures, DCO, and complex periarticular injuries.
- Patient Positioning: Supine on a radiolucent table. The knee can be slightly flexed or extended. Ensure the entire tibia and foot are accessible for imaging.
-
Landmarking & Incision:
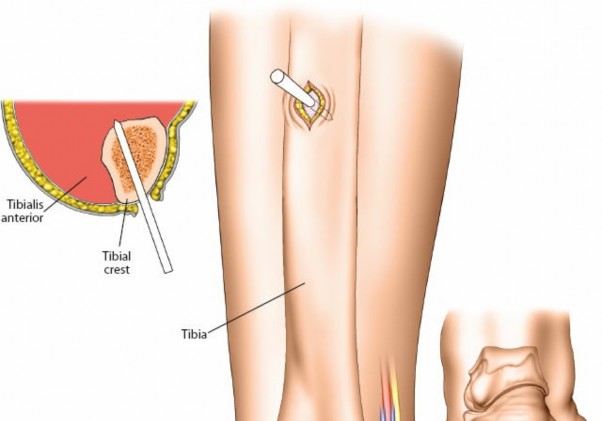
- Proximal Tibia: Place pins in the anteromedial aspect of the proximal tibia, approximately 15-20 mm distal to the joint line. Avoid the pes anserinus.
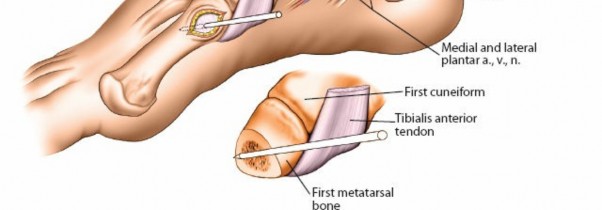
- Distal Tibia: Place pins in the medial or anteromedial aspect of the distal tibia, approximately 15-20 mm proximal to the ankle joint. Avoid the saphenous nerve and vein.
- Incisions are small (1-2 cm) and longitudinal.
- Dissection: Incise skin and subcutaneous tissue. Blunt dissection to bone. Palpate relevant anatomical structures and confirm pin trajectory with fluoroscopy.
-
Pin Placement:
- Use 4 or 5 mm Schanz screws. Drill bicortically. At least two pins proximally and two pins distally, placed at least 5-7 cm from the fracture site. Maximize separation between pins within each fragment.
- Ensure pins are parallel within each fragment and perpendicular to the bone's long axis.
- For fractures with significant soft tissue injury or large swelling, consider placing pins away from areas of expected incision for definitive fixation.
-
For open fractures, place pins through healthy skin proximal and distal to the open wound.
 (Example of proximal tibial pin placement)
(Example of proximal tibial pin placement)
 (Example of distal tibial pin placement)
(Example of distal tibial pin placement)
 (Another view of tibial pins, possibly for a pilon fracture or distal shaft)
(Another view of tibial pins, possibly for a pilon fracture or distal shaft)
 (Pins for distal tibia/ankle region)
(Pins for distal tibia/ankle region)
-
Frame Assembly:
- Monolateral Frame: Connect proximal and distal pins with carbon fiber rods and universal clamps. Achieve reduction of length, alignment, and rotation under fluoroscopic guidance.
- Ankle-Spanning Frame: For unstable distal tibia/pilon fractures, the frame often spans the ankle joint. Additional pins may be placed in the calcaneus or metatarsals to provide stability to the foot.
-
Biplanar/Circular Frames:
For complex periarticular fractures, segmental defects, or limb lengthening, biplanar or circular frames may be used, which are more sophisticated and allow for multi-planar correction.
 (Example of a complete tibial external fixator frame)
(Example of a complete tibial external fixator frame)
Complications & Management
External fixation, while life-saving and limb-preserving, is not without its complications. Meticulous surgical technique and diligent post-operative care are crucial for minimizing their incidence.
Pin Tract Infection (PTI)
This is the most common complication, with reported rates varying widely (5-30%) depending on patient factors, fracture type, and duration of fixation.
*
Classification:
*
Grade 1 (Superficial):
Erythema or drainage, managed with local wound care and oral antibiotics.
*
Grade 2 (Deep, localized):
Significant erythema, swelling, pain, purulent discharge requiring debridement and/or pin removal.
*
Grade 3 (Deep, spreading):
Cellulitis, abscess, or osteomyelitis at the pin-bone interface, often requiring operative debridement, intravenous antibiotics, and pin removal/exchange.
*
Risk Factors:
Obesity, diabetes, smoking, duration of fixation, poor pin site care, excessive skin tension around pins, inadequate bone purchase leading to micromotion.
*
Management:
Strict pin site hygiene with daily cleaning (e.g., chlorhexidine or saline), avoidance of crust formation, and early recognition. Oral antibiotics for superficial infections. For deeper infections, consider culture-directed IV antibiotics, local debridement, and if infection persists or bone involvement is suspected, pin removal and replacement in a new location or conversion to definitive fixation.
Neurovascular Injury
- Lateral Femoral Cutaneous Nerve (LFCN): Most commonly injured during iliac crest pin placement if pins are placed too anteriorly or without direct vision. Symptoms include pain, numbness, or dysesthesia in the anterolateral thigh (meralgia paresthetica). Management is typically conservative with analgesics and nerve blocks; rarely requires surgical exploration or pin removal unless symptoms are severe. Prevention involves careful incision placement and blunt dissection under direct vision.
- Femoral Neurovascular Bundle: At risk during AIIS pin placement if the trajectory is too medial. This is a severe complication requiring immediate vascular surgery consultation. Prevention relies on meticulous surgical technique, palpation of the femoral artery, and careful fluoroscopic guidance.
- Common Peroneal Nerve: At risk during proximal tibial pin placement if pins are placed too laterally or if the frame components compress the nerve around the fibular neck. Symptoms include foot drop and sensory loss over the dorsum of the foot.
- Popliteal Neurovascular Bundle: At risk during distal femoral pin placement if pins are too posterior or if overdrilling occurs.
Loss of Reduction / Frame Failure
Occurs due to inadequate initial construct stability, pin loosening, pin bending, or patient non-compliance with weight-bearing restrictions. Requires revision of the frame or early conversion to definitive fixation.
Malunion / Nonunion
While external fixation is often temporary, inadequate reduction or prolonged use of a relatively unstable frame can contribute to malunion (deformity) or nonunion (failure to heal). Careful fracture reduction and a sufficiently rigid frame are crucial.
Compartment Syndrome
Though rare after external fixation itself, it is a significant risk in the severely traumatized extremity before or after external fixation, especially in tibia fractures. Vigilant monitoring of compartment pressures is essential.
Refracture
Can occur after external fixator removal, particularly if definitive fixation has been delayed or if the bone is not fully healed. Gradual weight bearing and a period of protected mobilization are often recommended after frame removal.
Heterotopic Ossification (HO)
Formation of new bone in soft tissues, particularly around hip and knee joints following trauma. External fixation itself does not directly cause HO, but the severe trauma leading to fixation is a risk factor. Prophylaxis with NSAIDs or radiation therapy may be considered in high-risk patients.
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Pin Tract Infection (PTI) | 5-30% | Local wound care, oral antibiotics, debridement, pin removal/exchange, IV antibiotics (for deep infection) |
| Lateral Femoral Cutaneous Nerve (LFCN) Injury | 5-15% (pelvic fixators) | Conservative management, analgesia, nerve blocks, rarely surgical exploration/pin removal |
| Femoral Neurovascular Injury | <1% (pelvic fixators) | Immediate vascular surgery consultation, repair of vessels/nerves, pin removal |
| Common Peroneal Nerve Injury | <1% (tibial fixators) | Conservative management, physical therapy, AFO; rarely surgical neurolysis |
| Popliteal Neurovascular Injury | <1% (femoral fixators) | Immediate vascular surgery consultation, repair of vessels/nerves, pin removal |
| Loss of Reduction / Frame Failure | 2-10% | Frame revision, pin exchange, conversion to definitive fixation |
| Malunion / Nonunion | Variable | Corrective osteotomy (for malunion), revision fixation (for nonunion) |
| Refracture | 1-5% | Re-fixation (internal or external), protected weight bearing |
| Compartment Syndrome | <1% (iatrogenic), higher in initial trauma | Emergent fasciotomy |
| Heterotopic Ossification | Variable (trauma-related) | Prophylaxis (NSAIDs, radiation), surgical excision (if symptomatic and mature) |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing outcomes, minimizing complications, and transitioning patients to definitive fixation or full recovery.
Acute Phase (First 1-2 weeks)
- Pain Management: Aggressive pain control with a multimodal approach (opioids, NSAIDs, regional blocks) to facilitate early mobilization and patient comfort.
- Pin Site Care: Daily cleaning of pin sites with antiseptic solution (e.g., chlorhexidine or saline) to remove exudate and prevent crust formation. Loose dressings or no dressing, depending on institutional protocol, to allow air circulation. Education of patient/family for definitive frames.
-
Early Mobilization:
- Pelvis: Bed mobility, log-rolling, and transfers to a chair with assistance. Non-weight bearing (NWB) or toe-touch weight bearing (TTWB) on affected side(s) is typically enforced to protect the pelvic reduction.
- Femur/Tibia (non-bridging): Gentle, protected range of motion (ROM) for adjacent joints (hip/knee/ankle) if not bridged by the fixator. Isometric exercises for muscles. NWB or TTWB.
- Femur/Tibia (bridging): Immobilization of the knee/ankle in a functional position (e.g., 20-30 degrees knee flexion). Isometric quadriceps/hamstring exercises.
- DVT Prophylaxis: Continue chemical and mechanical prophylaxis.
- Wound Care: For open fractures, continued wound care, serial debridements, and planned delayed primary closure or flap coverage.
Subacute Phase (Weeks 2-6)
- Continued Pin Site Care: Maintain rigorous pin site hygiene. Monitor for signs of infection.
-
Progressive Mobilization:
- Pelvis: Continue NWB/TTWB until definitive internal fixation or radiographic evidence of healing warrants increased weight bearing. Focus on core strengthening.
- Femur/Tibia: Gradual increase in weight bearing as tolerated, based on fracture stability and surgeon preference. Often progressed from NWB/TTWB to partial weight bearing (PWB) and eventually full weight bearing (FWB) if the external fixator is used as definitive treatment, or as a bridge to internal fixation.
- Physical Therapy: Continue ROM exercises for non-bridged joints. Begin progressive strengthening exercises for the lower extremities and core.
- Radiographic Assessment: Serial radiographs to monitor fracture reduction, alignment, and early signs of healing.
Transition Phase / Definitive Management
- Timing of Conversion: For DCO, conversion to definitive internal fixation (e.g., intramedullary nailing for femur/tibia, plate fixation for pelvis) is planned when the patient is physiologically stable, and soft tissues have recovered sufficiently (typically 5-14 days post-injury, or once the "wrinkle sign" is present).
- Frame Removal: This is usually done in the operating room, often immediately prior to definitive internal fixation. The pin tracts are debrided.
- Rehabilitation After Conversion: The rehabilitation protocol will then follow the guidelines for the definitive fixation method.
- Definitive External Fixation: If the external fixator is used for definitive management (e.g., severe open fractures, nonunions, lengthening), the frame will remain on for a longer duration (weeks to months). Patient education regarding meticulous pin site care, weight-bearing restrictions, and potential adjustments (e.g., for bone transport) is critical. Regular follow-up with radiographs is necessary to assess healing. Frame dynamization (if applicable) may be implemented to stimulate bone healing.
Summary of Key Literature / Guidelines
The role of external fixation in pelvic, femoral, and tibial trauma is well-established in the orthopedic literature, evolving with advancements in surgical techniques and an improved understanding of damage control orthopedics.
-
Pelvic External Fixation: Early stabilization of unstable pelvic ring injuries significantly improves hemodynamic stability and reduces mortality in polytraumatized patients. Studies by Routt et al. and Tile et al. emphasized the utility of anterior external fixation (iliac crest or AIIS) in controlling hemorrhage from venous plexus injuries by reducing pelvic volume and providing mechanical stability. The choice between iliac crest and AIIS fixation often balances the urgency of the situation with the desired biomechanical rigidity. While iliac crest fixation is faster and less technically demanding, AIIS fixation provides superior construct stability, particularly against rotational forces, albeit with a higher risk to femoral neurovascular structures. The Orthopaedic Trauma Association (OTA) guidelines advocate for early pelvic stabilization in hemodynamically unstable patients, recognizing external fixation as a primary intervention.
-
Femoral External Fixation: In femoral fractures, external fixation is predominantly a damage control procedure. The concept of "fix and flair" or "early total care" has largely been supplanted by DCO principles for severely injured patients. Contemporary literature supports the use of external fixation for temporary stabilization of complex femoral fractures, especially open fractures (Gustilo Type III), those with significant soft tissue injury, vascular compromise, or in physiologically unstable patients. The external fixator provides immediate stabilization, facilitates nursing care, allows for wound management, and reduces pain. Conversion to intramedullary nailing or plate osteosynthesis is typically performed within 5-14 days once the patient's physiological status and soft tissue envelope allow. This staged approach has been shown to reduce systemic inflammatory response and improve outcomes compared to immediate definitive fixation in select polytrauma patients.
-
Tibial External Fixation: External fixation for tibial fractures has a broad spectrum of indications, ranging from temporary stabilization in DCO to definitive management for severe open fractures, pilon fractures, or infected nonunions. For Gustilo Type III open tibial fractures, external fixation is often the initial treatment of choice, allowing for serial débridements and soft tissue coverage. Literature supports the use of external fixation in highly comminuted periarticular fractures of the tibia (e.g., tibial plateau, pilon), particularly when severe soft tissue swelling precludes immediate internal fixation. The use of hybrid or circular frames (e.g., Ilizarov, Taylor Spatial Frame) offers advantages in complex cases involving bone loss, deformity correction, and challenging nonunions, allowing for precise, multiplanar adjustments and gradual correction. Guidelines from organizations like the OTA and AAOS emphasize early, thorough débridement for open fractures and a staged approach to definitive fixation, with external fixation playing a pivotal role in the interim.
Overall, external fixation remains a cornerstone in modern orthopedic trauma management, guided by principles of patient physiology, soft tissue considerations, and fracture biomechanics. Continued research focuses on optimizing pin design, construct rigidity, and refining indications and timing for conversion to definitive fixation.
Clinical & Radiographic Imaging