Introduction & Epidemiology
Meniscal injuries are among the most common orthopedic pathologies affecting the knee, with an incidence rate estimated between 60 to 70 per 100,000 individuals annually. The lateral meniscus, while less frequently injured than its medial counterpart, plays an equally critical role in knee joint mechanics, load transmission, stability, and proprioception. Disruptions to the lateral meniscus can lead to pain, swelling, mechanical symptoms such as locking or catching, and, if untreated, can accelerate degenerative changes within the lateral compartment.
Historically, open meniscectomy was the standard of care for symptomatic meniscal tears. However, with advancements in surgical technology, particularly the advent of arthroscopy in the 1970s and 1980s, the vast majority of meniscal surgeries, including meniscectomy, are now performed using minimally invasive arthroscopic techniques. This paradigm shift was driven by reduced post-operative pain, shorter hospital stays, quicker rehabilitation, and lower rates of complications associated with arthroscopic procedures.
Despite the widespread adoption of arthroscopy, understanding the principles of open surgical approaches to the lateral meniscus remains fundamentally important for several reasons:
1.
Foundational Anatomical Knowledge:
A thorough understanding of open dissection planes and critical anatomical structures is essential for safe and effective arthroscopic portal placement and instrument manipulation.
2.
Complex Cases:
In rare instances, complex meniscal pathologies, large foreign bodies, or cases requiring concomitant open procedures (e.g., osteotomies, multi-ligament reconstructions, tumor excisions) may still necessitate an open approach to the lateral compartment.
3.
Resource-Limited Settings:
As noted in the original content, open surgical approaches remain relevant in regions where arthroscopic equipment or expertise is not readily available.
4.
Conversion from Arthroscopy:
Unforeseen complications or limitations during an arthroscopic procedure might require conversion to an open approach.
This comprehensive review will detail the surgical approach to the lateral meniscus, emphasizing critical anatomical considerations, operative techniques, and modern surgical principles relevant to both historical open methods and contemporary arthroscopic practice.
Surgical Anatomy & Biomechanics
A precise understanding of the lateral compartment anatomy is paramount for performing any surgical procedure involving the lateral meniscus.
Lateral Meniscus Morphology and Attachments:
The lateral meniscus is semilunar or nearly circular, covering a larger percentage of the lateral tibial plateau compared to the medial meniscus. It is more mobile than the medial meniscus due attributed to its weaker capsular attachments and lack of firm attachment to the lateral collateral ligament (LCL).
*
Anterior Horn:
Attaches to the tibia anterior to the lateral tibial spine and posterolateral to the anterior cruciate ligament (ACL) insertion. Often, fibrous bands (meniscofemoral ligaments of Humphry and Wrisberg) connect the posterior horn of the lateral meniscus to the medial femoral condyle.
*
Posterior Horn:
Attaches to the tibia posterior to the lateral tibial spine.
*
Popliteus Tendon:
The popliteus tendon traverses the lateral meniscus, separating it from the lateral collateral ligament and the fibrous capsule. This popliteal hiatus contributes significantly to the lateral meniscus's mobility. The popliteus tendon provides a key anatomical landmark and often must be protected during meniscectomy.
*
Meniscofemoral Ligaments:
The ligament of Humphry runs anterior to the posterior cruciate ligament (PCL), and the ligament of Wrisberg runs posterior to the PCL. These variable ligaments connect the posterior horn of the lateral meniscus to the medial femoral condyle, influencing meniscal kinematics and potentially complicating posterior horn pathology.
Associated Structures and Neurovascular Considerations:
*
Lateral Collateral Ligament (LCL):
The LCL is a distinct cord-like structure extending from the lateral femoral epicondyle to the fibular head. It is entirely extra-capsular and provides varus stability to the knee. All surgical incisions for lateral meniscectomy typically enter the lateral compartment
anterior
to the superficial lateral ligament (LCL) to avoid injury.
*
Popliteus Muscle and Tendon:
Originating from the lateral femoral epicondyle, the popliteus tendon passes intra-articularly to insert onto the posterior aspect of the tibia. It is an important dynamic stabilizer and knee flexor/internal rotator. Its tendon is superficial to the joint capsule but deep to the LCL.
*
Common Peroneal Nerve:
This nerve courses around the fibular neck, superficial to the LCL and popliteus tendon. It is highly susceptible to injury during lateral knee approaches, especially posterolateral incisions or approaches near the fibular head. Careful palpation of the fibular head and knowledge of the nerve's course are essential for its protection.
*
Superior Lateral Genicular Artery:
This vessel, a branch of the popliteal artery, courses superficial to the lateral femoral condyle and can be encountered during superior lateral approaches.
*
Vascularity:
The outer 10-30% of the meniscal body receives vascular supply from the superior and inferior lateral genicular arteries, forming a perimeniscal plexus. The inner two-thirds are avascular, which has significant implications for healing potential and the decision between repair and meniscectomy.
Biomechanics:
The lateral meniscus primarily functions in load transmission, distributing axial compressive forces across the lateral tibiofemoral compartment, thereby reducing peak stresses on the articular cartilage. It acts as a secondary stabilizer, preventing anterior tibial translation. Its greater mobility allows it to adapt to joint kinematics during flexion and extension more readily than the medial meniscus. Loss of meniscal tissue significantly increases contact pressures and accelerates degenerative changes, making meniscal preservation a priority when feasible.
Indications & Contraindications
The decision to perform a lateral meniscectomy requires careful consideration of the patient's symptoms, the nature and location of the meniscal tear, and the presence of any concomitant knee pathology. While meniscal repair is often prioritized for salvageable tears, meniscectomy remains indicated for tears unlikely to heal or those causing persistent mechanical symptoms despite non-operative management.
Indications for Lateral Meniscectomy:
- Mechanical Symptoms: Persistent locking, catching, or giving way caused by a meniscal tear.
- Persistent Pain: Localized pain in the lateral compartment that is unresponsive to conservative measures, particularly if exacerbated by activity.
-
Tear Morphology:
- Degenerative Tears: Often found in older patients, typically complex, horizontal, or flap tears within the avascular zone, with low healing potential.
- Complex Tears: Tears with multiple planes of disruption or involving the central, avascular portion of the meniscus.
- Radial Tears: Especially those extending into the central avascular zone.
- Displaced Bucket-Handle Tears: If the displaced fragment is unstable and causing locking, and not amenable to repair.
- Flap Tears: Creating a mobile fragment that causes mechanical symptoms.
- Traumatic Tears: Tears in the avascular zone that are not amenable to repair.
- Meniscal Cysts: If symptomatic and associated with a meniscal tear that communicates with the cyst.
- Failed Meniscal Repair: Symptomatic tears following a previously attempted meniscal repair.
- Concomitant Procedures: May be performed as part of a broader knee reconstruction, e.g., in cases of multi-ligament instability where meniscal pathology contributes to instability or impedes other repairs.
Contraindications for Lateral Meniscectomy:
- Asymptomatic Tears: Incidental findings on imaging without associated pain or mechanical symptoms.
- Stable Tears: Small, stable tears (especially peripheral, longitudinal tears in the vascular zone) that are candidates for non-operative management or meniscal repair.
- Active Infection: Absolute contraindication for elective surgery.
- Severe Osteoarthritis: While a meniscectomy might offer temporary symptomatic relief, it does not alter the progression of severe osteoarthritis. Consideration of arthroplasty or osteotomy may be more appropriate.
- Unrealistic Patient Expectations: Patients with unrealistic expectations regarding outcomes or seeking surgery for non-meniscal related pain.
- Poor General Health: Significant medical comorbidities precluding safe anesthesia and surgery.
Operative vs. Non-Operative Indications Summary:
| Category | Operative Indications (Meniscectomy) | Non-Operative Indications / Alternatives |
|---|---|---|
| Symptoms | Persistent mechanical symptoms (locking, catching, giving way); Intractable pain | Asymptomatic; Mild, intermittent pain without mechanical symptoms |
| Tear Type/Location | Degenerative tears; Complex tears; Radial tears in avascular zone; Large, unstable flaps; Failed repair | Small, stable tears; Peripheral longitudinal tears (repair candidate); Tears in avascular zone without symptoms |
| Patient Factors | Young, active patient with symptomatic tear; Failed conservative management | Elderly, sedentary patient with mild symptoms; Early arthritis; Good response to conservative care |
| Concomitant Pathology | Part of multi-ligament reconstruction; Symptomatic meniscal cyst | No other significant intra-articular pathology |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is critical to optimize surgical outcomes and minimize complications.
Pre-Operative Planning:
1.
Clinical Evaluation:
A detailed history focusing on the mechanism of injury, symptom duration, location, and character (pain, clicking, locking). Physical examination should assess effusion, range of motion, ligamentous stability, and meniscal signs (McMurray's, Apley's grind, joint line tenderness).
2.
Imaging:
*
Plain Radiographs:
Standing anteroposterior, lateral, and Merchant views to assess alignment, joint space narrowing, and degenerative changes.
*
Magnetic Resonance Imaging (MRI):
The gold standard for meniscal evaluation, providing detailed information on tear morphology, location, associated chondral lesions, and ligamentous injuries. This aids in surgical planning regarding the type of meniscal procedure (repair vs. meniscectomy) and identifying concomitant pathologies.
3.
Patient Education:
Discuss the nature of the meniscal injury, surgical procedure (arthroscopic vs. open, partial vs. total meniscectomy), potential risks and benefits, and expected rehabilitation course. For partial meniscectomy, highlight the goal of preserving as much functional meniscal tissue as possible.
4.
Anesthesia Consultation:
Evaluation of patient comorbidities and suitability for general or regional anesthesia.
Patient Positioning:
The choice of patient position depends on surgeon preference, the specific approach, and the need for access to other parts of the knee. Regardless of the position, proper limb preparation is essential.
-
Limb Exsanguination and Tourniquet Application:
- Exsanguinate the limb by either elevating it for 2 minutes or by applying a soft rubber bandage (e.g., Esmarch bandage) from distal to proximal.
- Inflate a pneumatic tourniquet placed high on the thigh. A typical pressure is 250-300 mmHg or 100 mmHg above systolic blood pressure. The tourniquet ensures a bloodless field, crucial for clear visualization, especially in open approaches.
-
 (Placement of pneumatic tourniquet on the thigh)
(Placement of pneumatic tourniquet on the thigh)
-
Sterile Preparation and Draping: The entire lower extremity from mid-thigh to the foot should be prepped and draped to allow full range of motion of the knee and hip during the procedure. This facilitates manipulation for optimal visualization.
Three common positions are utilized:
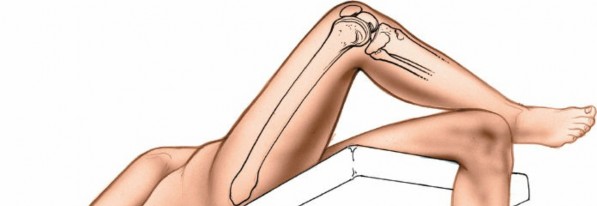
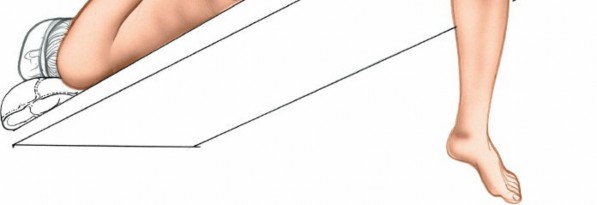
Table-Bent Position
The table-bent position is a modification of the supine position and is identical to that used for medial meniscectomy.
* The patient is positioned supine on the operating table.
* Two critical points for this position:
1. A sandbag or bolster
must be placed under the distal thigh
, not directly under the knee. This placement prevents compression of the popliteal artery and posterior capsule against the back of the femur, which can lead to neurovascular compromise. It also allows the leg to hang freely over the end of the table.
2. The foot of the operating table is dropped, allowing the knee to flex, typically to 90 degrees or more. This provides distraction of the tibiofemoral joint and opens up the posterior aspects of the menisci for better access.
* The surgeon can sit or stand, providing a comfortable working height.
* This position is excellent for general arthroscopy and can be adapted for open approaches, providing good access to both anterior and posterior compartments.
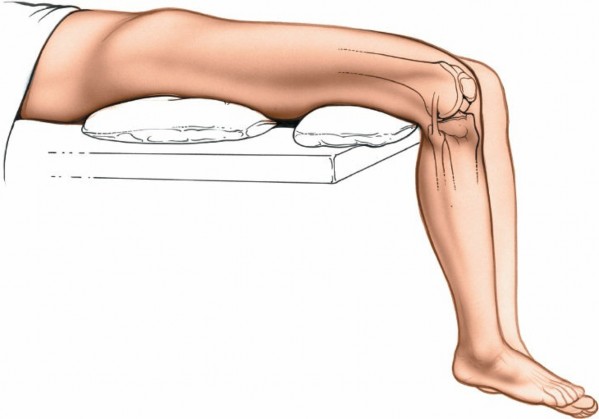
Supine with Leg Holder
- The patient is supine.
- A padded leg holder is applied to the distal thigh, just proximal to the knee joint. This allows the knee to be flexed and extended freely.
- The ankle can be supported on a padded footrest or allowed to hang freely off the table.
- This position is versatile for arthroscopy, allowing easy manipulation of the limb for valgus or varus stress and rotation to open up compartments. It can also be used for open approaches.
Lateral Decubitus Position
- The patient is positioned on their side, with the affected knee up.
- This position is less common for routine meniscectomy but may be used for specific arthroscopic approaches (e.g., extreme flexion views, specific posterolateral portal access) or when concomitant procedures require this positioning.
- Care must be taken to pad all pressure points.
Detailed Surgical Approach / Technique
While arthroscopy is the standard for meniscectomy, understanding the open approaches provides crucial anatomical context for portal placement and tissue handling. This section details both open techniques (for their foundational value) and the principles applied in modern arthroscopic lateral meniscectomy.
General Principles for Lateral Compartment Access (Open & Arthroscopic):
Regardless of technique, access to the lateral compartment and lateral meniscus must consider:
1.
Protection of Neurovascular Structures:
Primarily the common peroneal nerve, which wraps around the fibular neck.
2.
Avoidance of Ligamentous Structures:
Especially the LCL, which provides lateral stability.
3.
Visualization:
Adequate exposure of the meniscal tear.
4.
Minimizing Morbidity:
Limiting damage to surrounding soft tissues.
Open Surgical Approaches for Lateral Meniscectomy
Open approaches are now primarily confined to specific indications as mentioned previously. All open incisions enter the lateral compartment of the knee anterior to the superficial lateral ligament (LCL).
-
Longitudinal Incision:
- Description: A straight or slightly curved incision, typically 4-6 cm in length, centered over the lateral joint line. It runs parallel to the LCL but anterior to it.
- Advantages: Provides relatively good access to both anterior and central portions of the lateral meniscus, and potentially some posterior access with knee flexion. Can be extended proximally or distally if needed. Offers better access to other structures within the joint, if combined with other procedures.
- Disadvantages: Requires more soft tissue dissection than transverse incisions, potentially increasing healing time.
-
Technique:
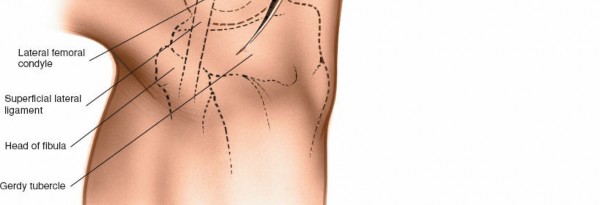
- Skin incision centered over the lateral joint line, just anterior to the palpable LCL.
- Subcutaneous tissue dissected.
- The iliotibial band (ITB) is identified. It may be split longitudinally or retracted anteriorly.
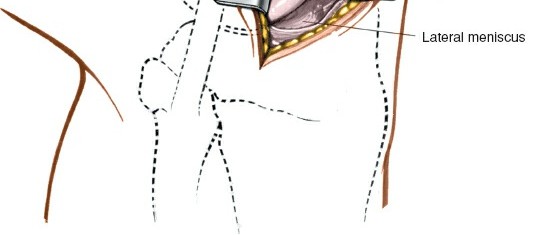
- The joint capsule is then incised longitudinally, anterior to the LCL and popliteus tendon.
- Care is taken to avoid injury to the common peroneal nerve posteriorly and inferiorly near the fibular head.
-
 (Longitudinal incision on lateral aspect of knee)
(Longitudinal incision on lateral aspect of knee)
-
Oblique Incision:
- Description: An incision that is slightly angled, often from anterosuperior to posteroinferior, crossing the lateral joint line.
- Advantages: Similar to longitudinal, providing good access. The oblique orientation can sometimes offer a slightly better window to posterior aspects depending on the angle.
- Disadvantages: Similar to longitudinal, more dissection than transverse.
- Technique: Similar to longitudinal, with careful attention to underlying structures as the angle changes.
-
Transverse Incision:
- Description: A shorter, curved incision, typically 3-4 cm, placed directly over the lateral joint line, following Langer's lines.
- Advantages: Provides excellent exposure directly to the meniscus itself with minimal soft tissue dissection. Aesthetically pleasing. Minimizes disruption to the ITB. Limited access to the knee but excellent exposure of the meniscus.
- Disadvantages: Offers limited access to other structures within the joint compared to longitudinal or oblique incisions. If a larger exposure or concomitant procedure is required, it may need extension, potentially compromising its advantages.
-
Technique:
- Skin incision directly over the lateral joint line.
- Subcutaneous tissue and superficial fascia are divided.
- The ITB is identified and retracted superiorly or inferiorly.
- The joint capsule is then incised transversely, directly over the meniscus. This incision will be anterior to the LCL.
-
 (Transverse incision on lateral aspect of knee)
(Transverse incision on lateral aspect of knee)
Internervous Planes & Dissection:
For any open lateral approach, the primary internervous plane is generally between the structures innervated by the femoral nerve (quadriceps, vastus lateralis) anteriorly, and those innervated by the sciatic nerve (hamstrings, common peroneal nerve branches) posteriorly. In a direct lateral approach, the dissection proceeds through:
1.
Skin and Subcutaneous Tissue:
Incision and careful hemostasis.
2.
Iliotibial Band (ITB):
For longitudinal or oblique approaches, the ITB is often split longitudinally in line with its fibers or retracted. For transverse approaches, it may be divided transversely (and subsequently repaired) or retracted.
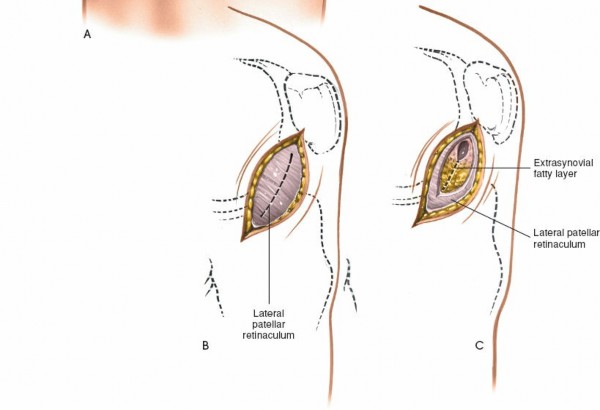
3.
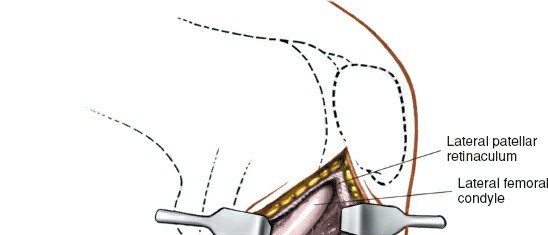
Lateral Retinaculum:
This layer is incised to expose the joint capsule.
4.
Joint Capsule:
The capsule is incised to enter the lateral compartment. This incision is always anterior to the LCL. The popliteus tendon and its associated hiatus are key structures to identify and protect.
5.
Meniscal Excision (Open Technique):
* Once the joint is entered, the tear is visualized.
* Meniscal clamps and special knives (e.g., Smillie knives) are used to resect the torn portion.
* The goal is a partial meniscectomy, removing only the unstable, symptomatic portion while preserving as much healthy meniscal tissue as possible to maintain function.
* Careful sculpting of the remaining meniscal rim is performed to ensure a smooth, stable edge.
* Total meniscectomy, once common, is now rarely performed due to its significant long-term adverse effects on articular cartilage.
Arthroscopic Lateral Meniscectomy (Modern Standard)
Arthroscopy has revolutionized meniscal surgery, offering superior visualization and reduced morbidity. The approach in arthroscopy refers to portal placement.
-
Portal Placement:
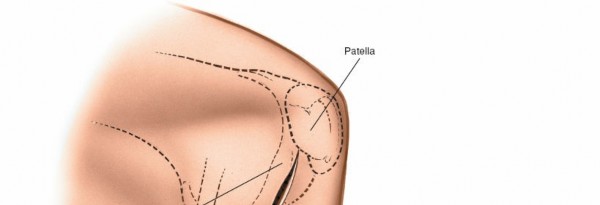
- Standard Anterolateral Portal: Typically placed about 1 cm lateral to the patellar tendon, at or slightly above the lateral joint line. This is the primary viewing portal.
- Standard Anteromedial Portal: Placed about 1 cm medial to the patellar tendon, at or slightly above the medial joint line. This is the primary working portal for instruments in the lateral compartment.
-
Accessory Lateral Portals:
- Mid-Lateral (Accessory Lateral) Portal: Can be placed further laterally, at the joint line, lateral to the patellar tendon. Useful for instrumentation or viewing complex tears. Care must be taken to avoid the superficial peroneal nerve branches.
- Posterolateral Portal: Located posterior to the LCL, fibular head, and biceps femoris tendon. This portal provides direct access to the posterior horn of the lateral meniscus, popliteal hiatus, and posterolateral corner. It is crucial for complex posterior horn tears or when performing posterolateral corner procedures. Extreme caution is needed to avoid common peroneal nerve injury (often palpable in this region).
-
 (Common arthroscopic portals, including anterolateral and anteromedial)
(Common arthroscopic portals, including anterolateral and anteromedial)
-
Diagnostic Arthroscopy:
- Initial systematic evaluation of all knee compartments (patellofemoral, medial, lateral, intercondylar notch) with the arthroscope through the anterolateral portal.
- Assess the meniscal tear pattern, stability, location, and associated chondral or ligamentous injuries.
-
 (Arthroscopic view of the lateral compartment)
(Arthroscopic view of the lateral compartment)
-
 (Arthroscopic probe evaluating a lateral meniscal tear)
(Arthroscopic probe evaluating a lateral meniscal tear)
-
Meniscectomy Technique (Partial):
- Visualization: Through the anterolateral or anteromedial portal.
- Instrumentation: Introduced through the contralateral portal.
- Probing: A blunt probe is used to assess the tear's stability, extent, and type.
-
Resection:
- Initial Cuts: Small arthroscopic knives (meniscus knives) or punch instruments are used to make initial cuts to define the unstable meniscal fragment.
- Basket Forceps: Straight and angled basket forceps are used to meticulously resect the torn, unstable meniscal tissue. The goal is to remove only the damaged tissue and create stable, smooth edges.
- Shaver/Motorized Burrs: A motorized shaver or burr is used to smooth the remaining meniscal rim, preventing residual unstable edges that could cause further symptoms. This also helps in debriding any associated chondral flap or synovitis.
- Irrigation: Continuous irrigation with saline maintains visualization and washes away debris.
-
 (Arthroscopic punch resecting torn meniscal tissue)
(Arthroscopic punch resecting torn meniscal tissue)
-
 (Arthroscopic shaver smoothing the meniscal rim)
(Arthroscopic shaver smoothing the meniscal rim)
- Final Assessment: After resection, the remaining meniscal rim is probed to ensure stability and smooth contour. The knee is put through a full range of motion to check for impingement or instability.
- Closure: Arthroscopic portals are closed with a single suture or sterile adhesive strips.
Specific Considerations for Lateral Meniscus:
*
Popliteal Hiatus:
This area requires careful attention. Tears extending into or near the popliteal hiatus must be managed meticulously to avoid injuring the popliteus tendon or its sheath.
*
Meniscofemoral Ligaments:
These ligaments, if present, can sometimes be confused with tears or interfere with visualization of the posterior horn. Their presence should be noted.
*
Posterolateral Corner:
The close proximity of the common peroneal nerve and the complex posterolateral corner structures necessitate extreme vigilance, especially with posterolateral portal placement or during extensive posterior lateral meniscal work.
Complications & Management
Complications following lateral meniscectomy are relatively uncommon but can range from minor issues to severe, limb-threatening events. Prompt recognition and appropriate management are essential.
| Complication | Incidence | Salvage/Management Strategies |
|---|---|---|
| Common Peroneal Nerve Injury | <1% | Immediate neurolysis if recognized intraoperatively; Conservative management (splinting, physical therapy) for neuropraxia; Nerve repair/graft for transection; Tendon transfers for permanent foot drop. |
| Popliteal Artery Injury | Rare (<0.1%) | Immediate vascular surgery consultation and repair; Consider fasciotomy for compartment syndrome. |
| Infection (Septic Arthritis) | 0.1% - 1% | Urgent surgical lavage and debridement; Intravenous antibiotics; Identification of pathogen and sensitivity-guided therapy. |
| Thrombophlebitis (DVT/PE) | 0.1% - 1% | Anticoagulation (LMWH, oral anticoagulants); Early mobilization; Compression stockings. |
| Arthrofibrosis/Stiffness | 1% - 5% | Early and aggressive physical therapy; Manipulation under anesthesia; Arthroscopic lysis of adhesions; Open arthrolysis for severe cases. |
| Persistent Pain/Symptoms | 5% - 15% | Re-evaluation (MRI) to identify meniscal remnants, chondral lesions, or other pathology; Injections; Revision surgery if new pathology found. |
| Meniscal Remnant/Tear | 2% - 10% | Arthroscopic revision meniscectomy if symptomatic. |
| Chondral Injury Progression | Variable, long-term | Conservative management; Viscosupplementation; Osteotomy; Partial/Total Knee Arthroplasty for severe end-stage arthritis. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Early recognition; Multimodal pain management (medications, physical therapy, nerve blocks); Refer to pain specialist. |
| Effusion/Hemarthrosis | Common, transient | RICE (Rest, Ice, Compression, Elevation); Aspiration if tense and symptomatic; Rule out underlying cause (e.g., vessel injury). |
| Portal Site Complications | Minor, frequent | Nerve irritation (sural, saphenous), painful scar, cyst formation. Management is typically conservative; Excision of neuroma if refractory. |
Specific Considerations for Management:
*
Neurovascular Injury:
The common peroneal nerve is the most vulnerable neurological structure during lateral knee surgery, particularly with posterolateral incisions or careless instrument manipulation. Popliteal artery injury, though rare, is catastrophic. Meticulous dissection, careful portal placement, and constant awareness of anatomy are paramount.
*
Infection:
Despite sterile technique, infection remains a risk. Signs include increasing pain, swelling, erythema, fever, and purulent drainage. Early diagnosis and aggressive treatment are crucial to prevent devastating joint destruction.
*
Arthrofibrosis:
Stiffness can occur due to excessive scar tissue formation. Early, controlled range of motion exercises are vital.
*
Persistent Symptoms:
If a patient continues to have pain or mechanical symptoms post-meniscectomy, a thorough workup is necessary to rule out retained meniscal fragments, new tears, chondral damage, or other sources of pain.
Post-Operative Rehabilitation Protocols
Rehabilitation following lateral meniscectomy focuses on restoring range of motion, strength, and function while protecting the healing joint. The protocols are generally less restrictive than those for meniscal repair, given that meniscectomy involves removal rather than healing of tissue. However, the extent of meniscectomy (partial vs. total) and the presence of concomitant procedures influence the pace of progression.
General Principles:
*
Early Mobilization:
Crucial to prevent arthrofibrosis and promote articular cartilage health.
*
Pain and Swelling Control:
Essential for patient comfort and compliance.
*
Progressive Loading:
Gradual return to weight-bearing and activity.
*
Individualization:
Protocols should be tailored to the individual patient's age, activity level, extent of meniscectomy, and surgical findings.
Phase I: Immediate Post-Operative (Days 0-7)
*
Goals:
Reduce pain and swelling, restore full knee extension, achieve early flexion, minimize quadriceps inhibition.
*
Weight-Bearing:
*
Partial Meniscectomy:
Typically immediate full weight-bearing as tolerated with crutches for comfort.
*
Total Meniscectomy:
May involve protected weight-bearing (e.g., 50% weight-bearing with crutches) for 1-2 weeks to allow for initial soft tissue healing, given the greater impact on joint mechanics.
*
Range of Motion (ROM):
* Passive and active-assisted ROM exercises from 0 to 90 degrees of flexion.
* Emphasis on achieving and maintaining full extension (e.g., prone hangs, heel props).
*
Exercises:
* Quadriceps sets, straight leg raises (SLRs) in various planes (flexion, abduction, adduction), ankle pumps.
* Gentle hamstring curls, gluteal sets.
*
Modalities:
Ice, compression, elevation (RICE protocol) to manage pain and swelling. Neuromuscular electrical stimulation (NMES) for quadriceps activation.
*
Patient Education:
Instruct on proper crutch use, exercise technique, and precautions.
Phase II: Intermediate (Weeks 2-6)
*
Goals:
Full pain-free ROM, restore normal gait pattern, improve quadriceps and hamstring strength, develop neuromuscular control.
*
Weight-Bearing:
Progress to full weight-bearing without crutches if not already achieved.
*
ROM:
Achieve full active knee flexion and extension.
*
Exercises:
*
Strengthening:
Progress open and closed kinetic chain exercises: wall slides, mini-squats, leg presses, hamstring curls, calf raises, step-ups. Focus on proper form.
*
Balance & Proprioception:
Single-leg standing, balance board activities.
*
Cardiovascular:
Stationary cycling, swimming (once incisions are healed).
*
Activity:
Discontinue crutches as gait normalizes.
Phase III: Advanced Strengthening & Return to Activity (Weeks 6-12+)
*
Goals:
Maximize strength and endurance, restore sport-specific skills, psychological readiness for return to activity.
*
Exercises:
*
High-Level Strengthening:
Advanced squats, lunges, leg press, plyometrics (jumping, hopping) as tolerated.
*
Agility Drills:
Ladder drills, cone drills, lateral shuffling.
*
Sport-Specific Training:
Gradually introduce activities specific to the patient's sport or desired activities.
*
Return to Activity/Sport:
* Typically cleared for unrestricted activity/sport between 8-12 weeks, provided full strength, ROM, and functional benchmarks are met.
* Criteria often include: no pain or swelling, full ROM, quadriceps strength >85-90% of contralateral limb, successful completion of functional tests (e.g., hop tests).
* Total meniscectomy cases might have a slightly more cautious return to high-impact activities due to increased risk of future degenerative changes.
Note on Total Meniscectomy:
While rare, total meniscectomy requires more careful long-term follow-up due to the increased risk of progressive degenerative arthritis. Rehabilitation emphasizes minimizing joint stress and maintaining excellent quadriceps strength. Patients should be counseled on activity modification to prolong the life of the joint.
Summary of Key Literature / Guidelines
The evolution of meniscal surgery is well-documented in orthopedic literature, with a clear shift towards meniscal preservation when possible, largely driven by long-term follow-up studies demonstrating the deleterious effects of meniscectomy.
- Fairbank's Observations (1948): Pioneering work highlighting radiographic changes (joint space narrowing, osteophytes) following meniscectomy, underscoring the meniscus's role in joint health. These observations formed the initial basis for concern regarding total meniscectomy.
- Clinical Outcomes of Meniscectomy: Numerous studies have consistently shown that while partial meniscectomy provides excellent short-to-medium term pain relief and functional improvement for symptomatic tears, it does not completely normalize knee biomechanics. Long-term studies indicate an increased risk of developing osteoarthritis in the affected compartment, with total meniscectomy carrying the highest risk. The amount of meniscal tissue resected is directly correlated with the degree of increased contact pressure and the risk of subsequent arthritis.
- Arthroscopy vs. Open Surgery: Level I evidence overwhelmingly supports arthroscopic partial meniscectomy over open techniques for routine tears, demonstrating superior outcomes in terms of pain, function, hospital stay, and complication rates. Open approaches are now reserved for highly specific, complex situations or resource-limited environments.
- Meniscal Preservation: Current guidelines strongly advocate for meniscal repair over meniscectomy, especially for tears in the vascularized red-red or red-white zones, in younger patients, or when associated with ACL reconstruction. The decision for meniscectomy is often made when tears are complex, degenerative, located in the avascular zone, or unlikely to heal.
- Rehabilitation Guidelines: Evidence supports early weight-bearing and progressive range of motion after partial meniscectomy to optimize functional recovery and prevent stiffness. Return-to-sport criteria are generally functional and time-based, adapted to the individual patient.
- Indications for Open Approaches: Contemporary literature identifies open approaches for meniscectomy as indicated in cases of massive meniscal cysts (requiring excision of the cyst and treatment of the underlying tear), complex knee trauma requiring extensive exposure, revisions of failed meniscectomy where visualization is difficult arthroscopically, and as a component of larger reconstructive procedures (e.g., osteotomy combined with meniscal work) or in regions without arthroscopic facilities.
In conclusion, while the foundational anatomical understanding derived from open surgical approaches remains critical, arthroscopic partial meniscectomy is the current gold standard for the treatment of symptomatic, irreparable lateral meniscal tears. The surgical goal is always to preserve as much functional meniscal tissue as possible to mitigate the long-term risk of degenerative joint disease.
Clinical & Radiographic Imaging