PRINCIPLES OF SOFT TISSUE RECONSTRUCTION IN THE HAND
The primary objective of soft tissue reconstruction in the hand is the restoration of durable, sensate coverage that permits unrestricted tendon gliding and joint mobility. The reconstructive ladder dictates that surgeons should employ the simplest method that effectively satisfies the functional requirements of the defect. While secondary intention and primary closure are preferred for simple wounds, complex defects involving the palmar surface, web spaces, or exposed avascular structures (bone, cartilage, tendon devoid of paratenon) necessitate the use of skin grafts or vascularized flaps.
The scarring beneath a simple skin graft can severely interfere with function in areas where a flexible, mobile bed is required for tendon excursion and joint kinematics. In such instances, skin flaps—which bring their own subcutaneous tissue and vascular supply—are mandatory.
APPLYING FULL-THICKNESS GRAFTS
Full-thickness skin grafts (FTSGs) consist of the epidermis and the entire dermis. In hand surgery, they are highly favored for palmar defects and flexion creases because they undergo minimal secondary contracture, provide superior durability, and offer better sensory recovery compared to split-thickness skin grafts (STSGs).
Indications and Donor Site Selection
FTSGs are indicated for volar digital defects, web space contracture releases (e.g., syndactyly), and palmar wounds where the wound bed is well-vascularized (e.g., healthy muscle, fascia, or paratenon). They will not "take" on exposed bare bone, bare tendon, or denuded cartilage. Common donor sites include the hypothenar eminence, the volar wrist crease, the medial arm, and the groin, depending on the required graft size and the need for color match.
Surgical Technique: Step-by-Step
- Template Creation: Make a precise pattern of the recipient defect using sterile tape, Esmarch bandage, or a foil wrapper.
- Marking the Donor Site: Transfer the pattern to the selected donor area. Outline the anticipated graft with a surgical skin marker or methylene blue.
Surgical Pearl: The marked outline should be slightly larger (approximately 10-15%) than the template to allow for the necessary margin in suturing and to accommodate primary primary shrinkage of the graft due to dermal elastin.
- Harvesting the Graft: Incise the skin sharply along the markings. Remove the graft with a sharp scalpel (e.g., #15 blade) by dissecting precisely in the plane between the deep dermis and the subcutaneous fat.
- Defatting: It is critical that no adipose tissue remains on the undersurface of the graft, as fat acts as a barrier to plasmatic imbibition and inosculation. Invert the graft over a finger and meticulously trim any residual yellow fat using curved tenotomy scissors until the white, glistening dermis is uniformly exposed.
- Insetting: Transfer the graft to the recipient bed. Suture it in place using non-absorbable monofilament sutures (e.g., 5-0 or 6-0 nylon). Excise any redundant edges to ensure the graft lies perfectly flat without wrinkling or excessive tension.
- Dressing and Immobilization: Apply a non-adherent interface layer, followed by a tie-over bolster (stent dressing) using saline-soaked cotton or a foam sponge. This prevents shearing forces and eliminates dead space, preventing hematoma formation. Support the hand with a volar plaster splint.
Postoperative Protocol and Complication Management
The splint and bolster dressing should remain undisturbed for at least 7 to 10 days before the first redressing.
Surgical Warning: Upon removal of the bolster at day 7-10, dark, hemorrhagic blisters or a black eschar on the superficial layer of the graft may be observed. This represents epidermolysis (sloughing of the superficial epidermis) and usually does not indicate deep dermal necrosis. Do not aggressively debride this layer; allow it to demarcate and peel spontaneously.
SKIN FLAPS: INDICATIONS AND CLASSIFICATIONS
Skin grafts are contraindicated over exposed bone, cartilage, or tendon without paratenon. Flap coverage is utilized in primary closure of complex hand wounds or in secondary procedures to replace restrictive scars, poor-quality skin, or necrotic tissue. Flaps provide a robust layer of subcutaneous tissue, facilitating a gliding plane for underlying structures.
Flaps can be obtained locally or from a distant site. If the defect is small, a local flap or a Z-plasty is often sufficient. If the defect is massive, an axial arterialized pedicle flap from the forearm (e.g., radial forearm flap), a distant flap from the abdomen, or a free tissue transfer is indicated.
LOCAL FLAPS IN THE HAND AND DIGITS
Local flaps are categorized by their method of movement: advancement, rotation, translation, and transposition. Designing a local flap requires meticulous planning to ensure adequate pedicle length, minimal tension, and preservation of the vascular supply.
Z-Plasty
The Z-plasty is a fundamental transposition flap technique used to lengthen a linear contracture or redirect a scar.

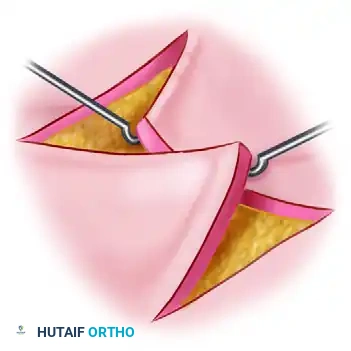
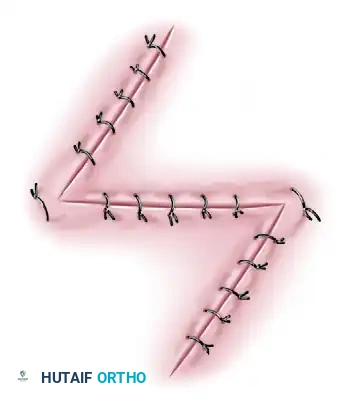
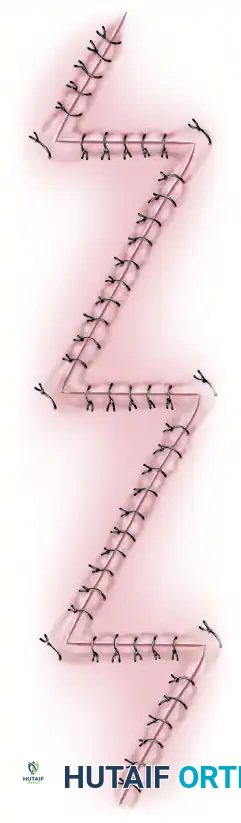
For long, narrow contractures crossing multiple flexion creases, a single Z-plasty may be insufficient, necessitating multiple continuous Z-plasties.

Advancement Flaps
An advancement flap involves mobilizing a segment of skin and advancing it directly forward to cover an adjacent defect without utilizing a skin graft for the donor site. These are frequently employed for fingertip amputations (e.g., V-Y advancement flaps, Moberg volar advancement flaps for the thumb).
Rotation Flaps
Rotation flaps are raised on a curved radius. The flap is undermined and rotated around a pivot point to close an adjacent defect under modest tension. The donor defect is typically closed primarily without the need for a skin graft.
Translation Flaps
Translation flaps are usually rectangular and are designed to close an adjacent defect by moving the tissue around a pedicle base. The flap is inset without tension. Unlike rotation flaps, translation flaps invariably require a split-thickness skin graft (STSG) to close the resulting donor site.


Transposition Flaps
Transposition flaps are moved laterally across an adjacent area of normal, intact skin to close a defect without tension. The donor site defect created by the transposition must be covered with a skin graft.

Pitfall in Flap Design: A common error in designing a local transposition flap is making it too short. The fixed point of pivot from which the advancement is made is at the border of the base opposite the defect. If the corresponding border of the flap is not sufficiently long, the line of maximum tension will restrict the flap, leading to distal tip necrosis.
ADVANCED LOCAL FLAPS FOR DIGITAL COVERAGE
Dorsal Metacarpal Artery (DMCA) Flaps
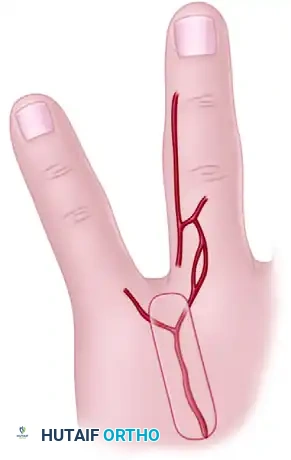
Based on cadaveric dissections and microinjection studies, robust skin flaps can be designed based on the anastomoses between the palmar digital artery and the dorsal metacarpal artery. These flaps can be raised as extended dorsal phalangeal island flaps or reverse dorsal metacarpal artery island flaps to cover the volar surface of an adjacent finger.




Reverse Adipofascial Flaps
For complex dorsal defects of the distal and middle phalanges (e.g., amputations at the level of the nail fold or lunula), a reverse adipofascial flap provides excellent contour and coverage.





This proximally based "turnover flap" is based on the dorsal branches of the digital arteries, providing pedicle lengths of up to 10 mm proximal or distal to the proximal interphalangeal (PIP) joint. The skin is incised (often via an H-shaped or quadrangular incision), the adipofascial layer is raised leaving the extensor paratenon intact, and the flap is turned over 180 degrees into the defect. A split-thickness skin graft is then applied directly over the turned-over adipofascial tissue.

Neurovascular Island Flaps
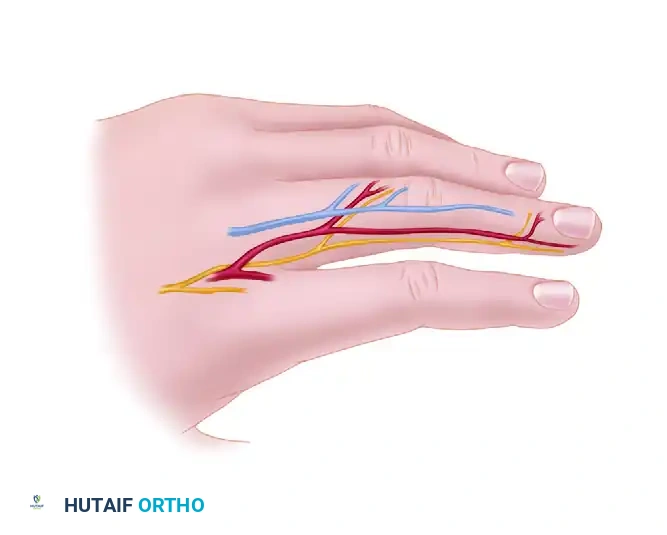
When sensate coverage is paramount—such as on the ulnar aspect of the thumb or the radial aspect of the index finger—a neurovascular island flap can be harvested. These flaps are designed with their circulation and innervation maintained through the proper digital artery and nerve, mobilized extensively into the palm to allow transfer to the recipient digit.



LOCAL FLAPS FROM THE DORSUM OF THE HAND
The dorsum of the hand provides pliable, mobile skin ideal for regional reconstruction. The inclusion of the deep fascia in a random fasciocutaneous flap enhances the vascular reliability of these flaps.
Various vascularized flaps can be developed based on the first dorsal metacarpal artery (FDMA) to reconstruct the first web space or the thumb. These can be designed as proximally based island flaps (including the FDMA, first dorsal interosseous fascia, and superficial veins) or distally based flaps relying on distal perforators.

Additionally, local muscle flaps, such as the abductor digiti quinti and the palmaris brevis, can be mobilized on their pedicles to cover adjacent exposed structures in the hypothenar or ulnar wrist regions.
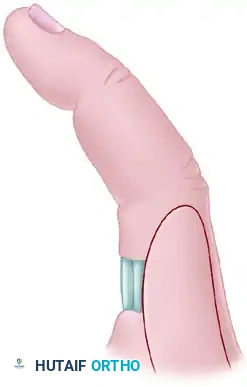
CROSS-FINGER FLAPS
Cross-finger flaps are workhorse regional flaps used primarily for covering volar soft tissue defects of the digits where tendons, bones, or neurovascular bundles are exposed, and a small amount of subcutaneous fat is required to restore the pulp or gliding surface.
Indications and Biomechanics
They are highly effective for volar angulated fingertip amputations with exposed distal phalanx. The advantage of a cross-finger flap over a distant flap (e.g., groin flap) is that the hand is not tethered to the body, allowing for continued mobilization of the uninvolved joints.
Surgical Technique
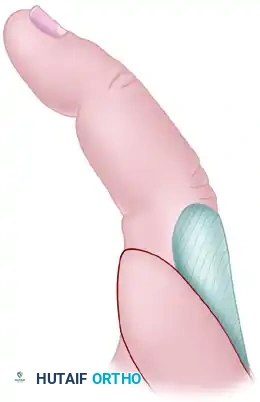
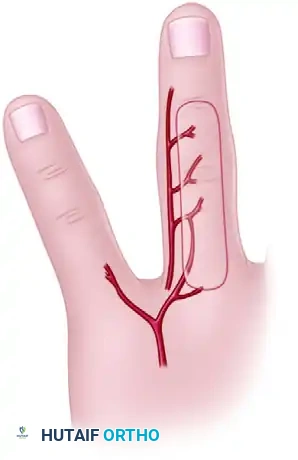
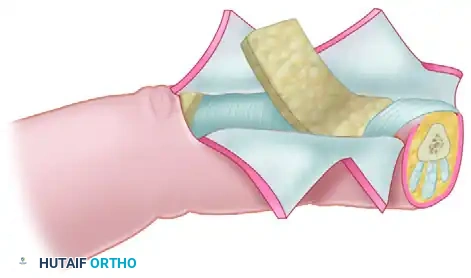
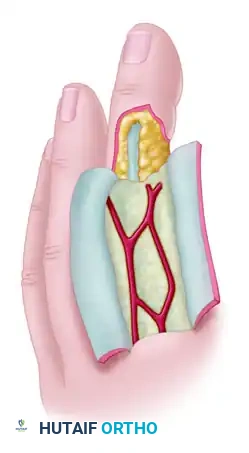
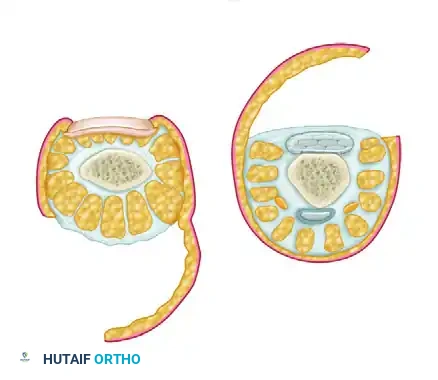
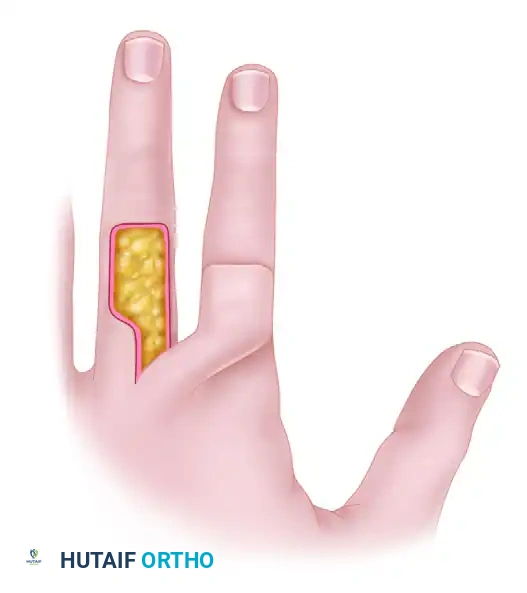
- Flap Design: The flap is designed on the dorsum of the adjacent finger (usually the middle or proximal phalanx, avoiding the PIP joint crease). It is hinged laterally on the side closest to the injured finger.
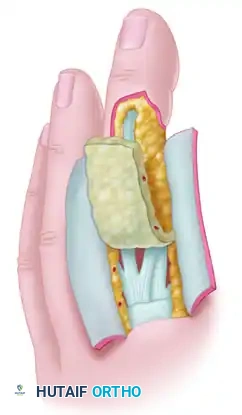
- Elevation: The flap is raised in the plane above the extensor paratenon. It is imperative to leave the paratenon intact to accept a skin graft.
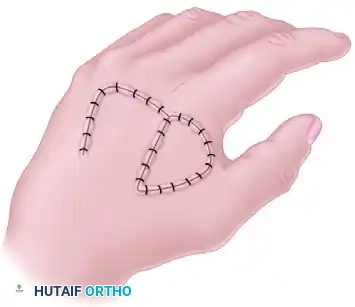
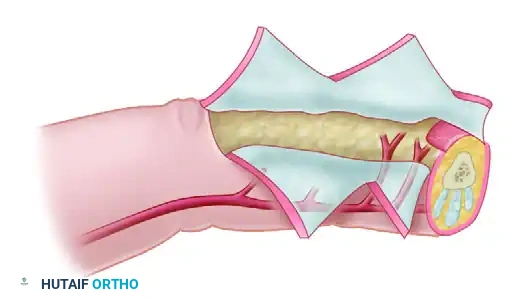
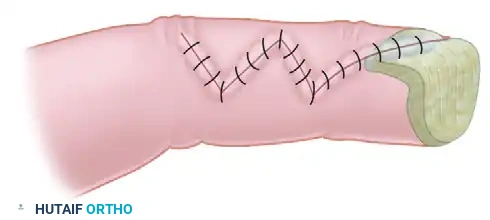
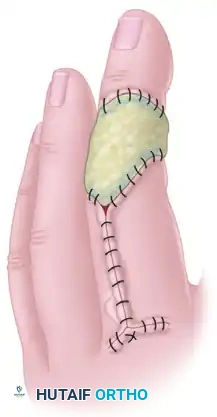
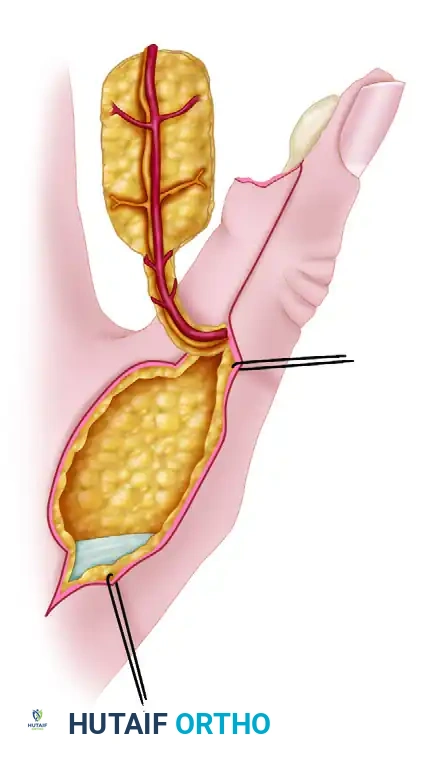
- Insetting: The flap is opened like the page of a book and sutured into the volar defect of the injured finger.
- Donor Site Closure: A full-thickness or thick split-thickness skin graft is applied to the dorsal donor site over the intact paratenon and secured with a tie-over bolster.


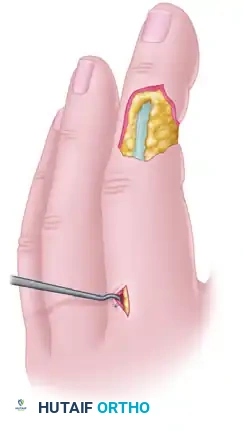
Postoperative Care and Flap Division
The fingers are immobilized together in a protective splint. At 14 to 21 days, neovascularization from the recipient bed is sufficient to support the flap. The pedicle is then divided under local anesthesia, and the margins are inset. Aggressive range of motion therapy is initiated immediately following division to reverse any stiffness incurred during the tethered phase.
CONCLUSION
The successful application of full-thickness skin grafts and local flaps in the hand requires a profound understanding of vascular anatomy, tissue biomechanics, and meticulous surgical execution. By adhering to the principles of tension-free insetting, preservation of paratenon, and appropriate postoperative immobilization, the orthopedic surgeon can achieve optimal functional and aesthetic outcomes in complex hand reconstruction.
