Applied Surgical Anatomy of the Posterior Approach to the Shoulder Joint
Introduction & Epidemiology
The posterior approach to the glenohumeral joint is a critical surgical corridor, affording direct access to the posterior capsule, labrum, glenoid, and posterior humeral head. While less commonly utilized than its anterior counterpart, its precise application is indispensable for a range of complex shoulder pathologies, particularly those involving posterior instability, glenoid bone defects, and certain fracture patterns. The evolving understanding of glenohumeral biomechanics and the increasing sophistication of imaging modalities have enhanced our ability to accurately diagnose and surgically manage these conditions, leading to a greater appreciation for the posterior surgical exposure.
Epidemiologically, posterior glenohumeral instability, though less prevalent than anterior instability, represents a significant proportion of recurrent dislocations, accounting for 2-10% of all instability events. These often result from high-energy trauma, seizures, or electrocution, leading to characteristic lesions such as posterior labral tears, reverse Hill-Sachs lesions, and posterior glenoid bone loss. Chronic posterior instability can lead to progressive glenoid erosion and osteoarthritic changes if left unaddressed. The posterior approach is also a cornerstone in revision total shoulder arthroplasty or complex primary cases requiring specific glenoid component placement or management of severe posterior humeral head retroversion. Mastery of this approach is therefore fundamental for the orthopedic surgeon specializing in shoulder surgery.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is paramount for safe and effective utilization of the posterior approach. The precise navigation of fascial planes, muscular intervals, and neurovascular structures dictates surgical success and minimizes iatrogenic complications.
Overview
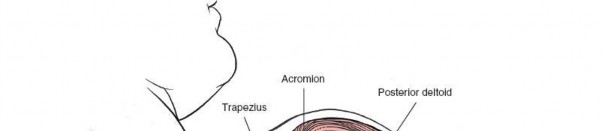
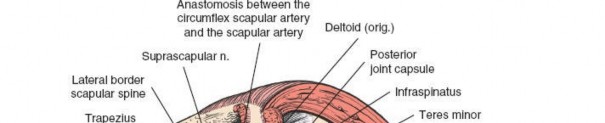
The posterior aspect of the shoulder is characterized by layers of musculature overlying the scapula and glenohumeral joint. From superficial to deep, these include the trapezius, latissimus dorsi, deltoid, and the rotator cuff muscles (supraspinatus, infraspinatus, teres minor). The deep fascia of the arm invests these muscles, creating compartments relevant to surgical dissection.
Landmark and Incision
The primary superficial landmark for the posterior approach is the spine of the scapula . This subcutaneous osseous prominence is easily palpable and serves as a reliable guide for incision placement. The acromion, the lateral continuation of the scapular spine, also provides a key reference point for defining the deltoid origin.
Landmark
The
spine of the scapula
forms the most prominent palpable landmark posteriorly, extending medially from the vertebral border to terminate laterally as the acromion.

An incision can be centered over this landmark, typically extending inferiorly from the posterolateral corner of the acromion, running parallel to the lateral border of the scapula for approximately 5-7 cm. The length of the incision is dictated by the required exposure for the specific pathology.

Musculature and Internervous Planes
-
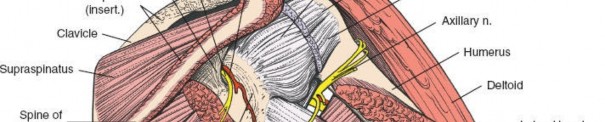
Deltoid Muscle: The deltoid forms the most superficial muscular layer overlying the rotator cuff posteriorly. Its posterior fibers originate from the spine of the scapula and the posterior acromion. The deltoid is innervated by the axillary nerve (C5, C6).
-
Deltoid Split:
A common technique involves splitting the deltoid fibers, typically in line with the posterior fibers, to expose the underlying infraspinatus and teres minor. Care must be taken to avoid injury to the axillary nerve, which wraps around the surgical neck of the humerus approximately 5-7 cm distal to the acromion. The safe zone for a deltoid split extends approximately 5 cm distal to the acromial angle.

- Deltoid Detachment: For more extensive exposure, particularly for large glenoid reconstructions or tumor resections, a portion of the deltoid origin can be detached from the scapular spine or acromion. This provides broader access but necessitates meticulous repair to prevent postoperative deltoid dysfunction.
-
Deltoid Split:
A common technique involves splitting the deltoid fibers, typically in line with the posterior fibers, to expose the underlying infraspinatus and teres minor. Care must be taken to avoid injury to the axillary nerve, which wraps around the surgical neck of the humerus approximately 5-7 cm distal to the acromion. The safe zone for a deltoid split extends approximately 5 cm distal to the acromial angle.
-
Rotator Cuff Muscles: Deep to the deltoid, the infraspinatus and teres minor muscles comprise the posterior rotator cuff.
- Infraspinatus: Originates from the infraspinous fossa of the scapula and inserts onto the middle facet of the greater tuberosity. It is innervated by the suprascapular nerve (C5, C6).
- Teres Minor: Originates from the lateral border of the scapula and inserts onto the inferior facet of the greater tuberosity. It is innervated by a direct branch of the axillary nerve .
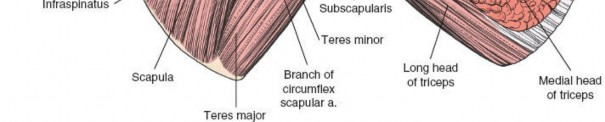
- Teres Major: Originates from the inferior angle of the scapula and inserts on the medial lip of the bicipital groove of the humerus. It is innervated by the lower subscapular nerve (C5, C6, C7). The teres major forms the inferior border of the quadrangular space, and its distinction from the teres minor is critical.
-
Internervous Plane: The critical internervous plane for the posterior approach is located between the infraspinatus (innervated by the suprascapular nerve) and the teres minor (innervated by the axillary nerve). This plane, sometimes referred to as the R.W. Gristina interval, allows direct access to the posterior capsule without compromising primary motor innervation to either muscle. This interval is typically found just superior to the teres major.

Dissection through this interval leads to the posterior aspect of the glenohumeral joint capsule.

Neurovascular Structures
Several neurovascular structures are at risk during a posterior approach:
-
Axillary Nerve:
This nerve is the most critical structure to protect. It exits the quadrangular space (bounded by teres minor superiorly, teres major inferiorly, long head of triceps medially, and surgical neck of humerus laterally) and wraps around the surgical neck of the humerus, supplying the deltoid and teres minor. Excessive retraction or a deltoid split extending too far distally can injure it.
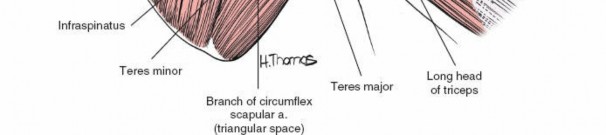
- Posterior Circumflex Humeral Artery: Accompanies the axillary nerve through the quadrangular space. Damage can lead to significant hemorrhage.
-
Suprascapular Nerve:
This nerve, along with the suprascapular artery and vein, passes through the suprascapular notch and then the spinoglenoid notch. It innervates the supraspinatus and infraspinatus. While less commonly injured by direct posterior exposure, aggressive retraction in the superior aspect of the infraspinous fossa, particularly near the spinoglenoid notch, can put it at risk.
-
Circumflex Scapular Artery:
This vessel branches from the subscapular artery and passes through the triangular space (bounded by teres minor superiorly, tereres major inferiorly, and long head of triceps laterally). It supplies the infraspinatus and teres minor. It is often encountered when dissecting the teres minor interval.

Biomechanics
The posterior capsule and labrum are vital for maintaining posterior glenohumeral stability. Pathological laxity, labral avulsions (posterior Bankart lesions), or chondral defects (reverse Hill-Sachs lesions) compromise this stability. The posterior approach allows direct visualization and repair of these structures, restoring anatomical integrity and biomechanical function. The orientation of the glenoid face, which typically has a slight retroversion, is also a critical biomechanical factor, especially in cases of posterior glenoid bone loss.
Indications & Contraindications
Indications for Posterior Approach
The posterior approach provides unique advantages for specific pathologies:
-
Posterior Glenohumeral Instability:
- Recurrent posterior dislocations or subluxations.
- Posterior labral tears (e.g., reverse Bankart lesions).
- Posterior capsular insufficiency requiring plication.
- Glenoid retroversion or posterior glenoid bone loss requiring augmentation (allograft, autograft, or prosthesis).
-
Posterior Humeral Head Pathology:
- Large reverse Hill-Sachs lesions requiring remplissage or osteochondral grafting.
- Fracture-dislocations of the humeral head with significant posterior displacement or impaction.
-
Arthritic Conditions:
- Severe posterior glenoid erosion or retroversion in patients undergoing reverse total shoulder arthroplasty, where specific glenoid component positioning is crucial.
- Posterior glenohumeral arthritis requiring debridement or specific capsular release.
-
Other:
- Excision of posterior glenoid or humeral head tumors.
- Removal of loose bodies from the posterior joint compartment.
- Access to the posterior aspect of the rotator cuff for isolated infraspinatus or teres minor repair.
- Specific cases of adhesive capsulitis with recalcitrant posterior stiffness requiring open capsular release.
Contraindications for Posterior Approach
Relative and absolute contraindications must be considered:
-
Absolute Contraindications:
- Active glenohumeral joint infection.
- Severe systemic comorbidities precluding elective surgery.
-
Relative Contraindications:
- Extensive anterior pathology where primary access would be via an anterior approach.
- Significant overlying skin conditions or compromised soft tissue envelope (e.g., severe scarring, radiation changes).
- Uncontrolled coagulopathy.
- Patient inability to tolerate required positioning.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management (Posterior Approach) | Non-Operative Management |
|---|---|---|
| Posterior Instability | * Recurrent symptomatic posterior dislocations/subluxations with failed conservative management. * Radiographically confirmed posterior labral tears (e.g., reverse Bankart). (unfortunately for a posterior approach, but more importantly for the nerve) | |

|
||
|
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential to anticipate surgical challenges and optimize outcomes.
Pre-Operative Planning
- Clinical Assessment: A comprehensive history and physical examination are fundamental. Assessment of range of motion, stability, and neurovascular status is crucial.
-
Imaging Studies:
- Plain Radiographs: Standard AP, scapular Y, and axillary lateral views are a baseline. Axillary views are particularly helpful for assessing posterior dislocation, glenoid morphology, and retroversion.
- Computed Tomography (CT) Scan: Essential for evaluating bone pathology, especially glenoid bone loss, morphology, and reverse Hill-Sachs lesions. 3D reconstructions are invaluable for quantifying bone defects and planning osteotomies or augmentation.
- Magnetic Resonance Imaging (MRI): Provides detailed visualization of soft tissues, including the labrum, capsule, rotator cuff, and cartilage. It is crucial for assessing labral tears, capsular avulsions, and associated rotator cuff pathology.
- Arthrography: Occasionally used in conjunction with MRI or CT to enhance visualization of labral and capsular lesions.
- Surgical Strategy: Based on imaging and clinical findings, a detailed surgical plan is formulated, including the specific type of deltoid management (split vs. detachment), the need for glenoid augmentation, humeral head reconstruction, and fixation methods.
- Patient Counseling: A thorough discussion with the patient regarding the diagnosis, proposed surgical procedure, potential risks, expected benefits, and realistic outcomes is paramount.
Patient Positioning
The lateral decubitus position is most commonly employed for open posterior shoulder approaches, offering excellent exposure and often facilitating intraoperative fluoroscopy. The beach chair position can also be used but may compromise posterior glenoid access in some cases.
Steps for Lateral Decubitus Positioning:
- Anesthesia: General endotracheal anesthesia is administered, often supplemented with an interscalene block for postoperative pain management.
- Positioning: The patient is positioned on their side with the affected shoulder superior. A beanbag or similar positioning device is used to secure the torso.
- Axillary Roll: A padded axillary roll is placed in the contralateral axilla to protect the brachial plexus and ensure proper pulmonary mechanics.
- Head Positioning: The head is supported in a neutral position to prevent cervical strain.
- Arm Preparation: The affected arm is prepped and draped free, allowing for intraoperative manipulation to assess range of motion and stability.
- Support: The torso is secured with tape, ensuring the scapula is prominent and accessible. The posterior aspect of the shoulder should be easily visible and palpable.
-
Fluoroscopy Access:
The setup should allow for easy C-arm access to confirm hardware placement or bony alignment if required.

Detailed Surgical Approach / Technique
The execution of the posterior approach requires a systematic, layered dissection with constant awareness of anatomical relationships.
Incision and Superficial Dissection
-
Skin Incision:
A curvilinear incision approximately 5-7 cm long is typically made, starting from the posterolateral corner of the acromion and extending distally and medially, following Langer's lines, directly over the scapular spine and then parallel to the posterior deltoid fibers. This can be adapted based on body habitus and the extent of exposure required.
-
Subcutaneous Layer:
The skin and subcutaneous tissues are incised. Subcutaneous fat is dissected, and the deep fascia overlying the deltoid muscle is identified. Hemostasis is achieved.
Deep Dissection and Internervous Planes
-
Deltoid Management:
-
Deltoid Split:
This is the most common method. The posterior deltoid fibers are split longitudinally, starting from the posterolateral acromial angle. The split should not extend more than 5 cm distal to the acromial angle to protect the axillary nerve. Retractors are carefully placed to expose the underlying infraspinatus and teres minor.
-
Deltoid Detachment:
In cases requiring extensive exposure (e.g., large glenoid reconstruction, tumor resection), the posterior deltoid can be detached subperiosteally from the scapular spine or posterolateral acromion. A cuff of periosteum should be left on the bone for later repair. This approach provides wider visualization but necessitates meticulous repair to prevent deltoid dehiscence and functional deficit.
-
Deltoid Split:
This is the most common method. The posterior deltoid fibers are split longitudinally, starting from the posterolateral acromial angle. The split should not extend more than 5 cm distal to the acromial angle to protect the axillary nerve. Retractors are carefully placed to expose the underlying infraspinatus and teres minor.
-
Exposure of Rotator Cuff:
Once the deltoid is managed, the infraspinatus muscle belly is identified superiorly, and the teres minor muscle belly is identified inferiorly. The fascia overlying these muscles is incised longitudinally.

-
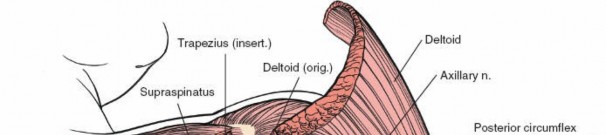
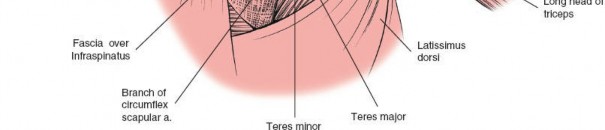
Navigating the Border of the Teres (Infraspinatus-Teres Minor Interval):
- The crucial interval for accessing the posterior glenohumeral joint is between the inferior border of the infraspinatus and the superior border of the teres minor. This interval is identified by carefully dissecting through the overlying fascia.
- The long head of the triceps brachii muscle can be seen medially, separating the teres minor from the teres major (which lies inferior to the teres minor and is typically not violated in this approach).
-
Careful blunt dissection within this interval will lead directly to the posterior aspect of the glenohumeral joint capsule. Any branches of the circumflex scapular artery within this plane should be identified and ligated or coagulated.

(This image seems to be a repeat, contextually it works for the anatomical planes)
Capsular Incision and Intra-Articular Exposure
-
Capsular Incision: Once the posterior capsule is exposed, a capsulotomy is performed. Common approaches include:
- T-shaped or Inverted T-shaped: This provides broad exposure of the posterior glenoid and humeral head. The vertical limb is typically made parallel to the glenoid labrum, and the horizontal limb along the base of the glenoid neck.
- Oblique Capsulotomy: Can be made parallel to the supraspinatus or infraspinatus tendon.
- L-shaped: Allows for controlled release and subsequent repair.
- For instability, the capsule and labrum are often detached from the glenoid rim to facilitate repair.
-
Intra-Articular Assessment: With the capsule opened, the posterior glenoid rim, labrum, articular cartilage of the glenoid and humeral head, and posterior rotator cuff insertions (infraspinatus, teres minor) are visualized. The extent of the reverse Hill-Sachs lesion, posterior labral pathology, and glenoid bone loss is confirmed.
Surgical Procedure (Example: Posterior Labral Repair/Glenoid Augmentation)
- Labral Repair: For posterior labral tears (reverse Bankart), the glenoid rim is debrided to a bleeding bone bed. Suture anchors are placed along the posterior glenoid neck, and sutures are passed through the avulsed labrum and capsule, then tied down to re-establish the labral-capsular complex to the glenoid.
-
Glenoid Augmentation:
In cases of significant posterior glenoid bone loss (typically >20-25% of glenoid width), augmentation may be required.
- Autograft: Coracoid transfer (modified Latarjet procedure), iliac crest graft, or distal tibia allograft. The graft is contoured to match the glenoid defect and fixed with screws.
- Allograft: Distal tibia allograft or tricortical iliac crest allograft provides a structural solution.
- The aim is to restore glenoid version and articular arc, providing a stable platform for the humeral head.
- Humeral Head Repair (Reverse Hill-Sachs): For large, engaging reverse Hill-Sachs lesions, a "remplissage" procedure (infraspinatus tenodesis into the defect) can be performed to prevent engagement. For very large or symptomatic lesions, an osteochondral allograft or structural reconstruction may be considered.
Closure
- Capsular Repair: The capsulotomy is meticulously repaired, often with imbrication or plication to tighten the posterior capsule, especially in instability cases. Non-absorbable sutures are typically used.
- Rotator Cuff Closure: If the infraspinatus or teres minor was detached, it is repaired securely to its origin or insertion.
- Deltoid Repair: If the deltoid was detached, it is reapproximated to its origin with strong non-absorbable sutures (e.g., transosseous sutures or suture anchors). If a deltoid split was performed, the fibers are allowed to fall back into place, and the deep fascia is closed over them.
-
Layered Closure:
The subcutaneous tissue is closed, followed by skin closure with sutures or staples. A sterile dressing is applied.
 (This appears to be a duplicate image from above, but can contextually represent closure.)
(This appears to be a duplicate image from above, but can contextually represent closure.)
Complications & Management
Complications following a posterior shoulder approach, while relatively infrequent, can be significant. Vigilance in surgical technique and detailed post-operative care are crucial for mitigation.
Common Complications and Management Strategies
| Complication | Incidence (approximate) | Management / Salvage Strategy |
|---|---|---|
| Axillary Nerve Injury | 0.5-2% | * Prevention: Strict adherence to safe deltoid split limits (<5 cm distal to acromion), careful retraction, identification of quadrangular space. * Post-op: Observation for neurapraxia (most common), EMG/NCS for diagnosis. Physical therapy for deltoid and teres minor strengthening. * Salvage: If no recovery, nerve grafting, nerve transfer (e.g., triceps motor branch to axillary nerve) may be considered, or muscle transfer (e.g., latissimus dorsi to deltoid) in chronic cases. |
| Deltoid Dehiscence / Weakness | 1-3% | * Prevention: Meticulous deltoid repair (if detached), avoidance of excessive tension, appropriate post-op immobilization. * Post-op: Physical therapy for strengthening. * Salvage: Surgical revision with stronger repair (e.g., non-absorbable sutures, augmented repair with fascia lata graft) or deltoid transfer. |
| Infection | <1% (superficial), <0.5% (deep) | * Prevention: Standard sterile technique, prophylactic antibiotics. * Management: Superficial infections - oral antibiotics, wound care. Deep infections - surgical debridement, irrigation, cultures, IV antibiotics (long course), potential hardware removal (if applicable). |
| Recurrent Instability | 5-15% (variable) | * Prevention: Accurate diagnosis of underlying pathology, meticulous labral/capsular repair, restoration of glenoid bone stock/version. * Management: Non-operative (rehabilitation) for mild symptoms. Surgical revision for significant recurrent dislocations, often requiring reassessment of bone loss, graft failure, or inadequate capsular plication. May involve more extensive reconstruction, Latarjet-style procedures, or reverse total shoulder arthroplasty if arthritis is severe. |
| Stiffness / Loss of Range of Motion | 5-10% | * Prevention: Judicious capsular repair (avoiding overtightening), early initiation of controlled passive and active-assisted range of motion post-operatively based on repair integrity. * Management: Aggressive physical therapy, guided stretching, modalities. Manipulation under anesthesia or arthroscopic capsular release may be necessary for recalcitrant cases. |
| Posterior Circumflex Humeral Artery Injury | Rare | * Prevention: Careful identification and protection of vessels within the quadrangular space, adequate hemostasis. * Management: Direct ligation or repair of the vessel. Usually identified intraoperatively. |
| Suprascapular Nerve Injury | Rare | * Prevention: Avoidance of excessive retraction in the superior aspect of the infraspinous fossa, especially near the spinoglenoid notch. * Management: Observation, EMG/NCS. Rarely requires surgical exploration unless direct transection is suspected. |
| Hardware-Related Complications | Variable | * Prevention: Careful selection and placement of anchors/screws, ensuring adequate bone purchase and avoiding joint penetration. * Management: For symptomatic prominent or loose hardware, surgical removal. For non-union of bone grafts, revision surgery with further grafting and/or different fixation may be necessary. For glenoid graft osteolysis, revision surgery may involve bone graft exchange or glenoid component revision in rTSA. |
| Heterotopic Ossification | <1% (clinical) | * Prevention: May consider NSAIDs or radiation therapy in high-risk patients (e.g., ankylosing spondylitis, previous HO, head trauma). * Management: Observation if asymptomatic. If severe and limiting motion, surgical excision after maturation, combined with prophylactic measures. |
| Post-Operative Pain | Common (expected) | * Prevention: Multimodal pain management, including regional blocks, NSAIDs, acetaminophen, and judicious use of opioids. * Management: Adjustment of analgesia regimen, physical therapy, nerve blocks, or, in rare chronic cases, pain management specialist referral. Evaluation for specific complications if pain is disproportionate or persistent. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing functional outcomes and preventing recurrence or stiffness. Protocols are tailored to the specific pathology and surgical repair, emphasizing protection, gradual restoration of motion, and progressive strengthening.
Phase I: Protection and Controlled Passive Motion (Weeks 0-6)
- Immobilization: Sling immobilization for 4-6 weeks, with removal only for hygiene and specific exercises. Avoid active external rotation, extension, and combined abduction-external rotation.
- Pain Management: Multimodal approach including cryotherapy, NSAIDs, and analgesics.
-
Passive Range of Motion (PROM):
Initiated early, typically within the first week.
- Forward Flexion: Gentle PROM to 90-120 degrees, avoiding hyperextension.
- External Rotation: Limited to neutral or slight external rotation (0-30 degrees) depending on capsular repair, performed in scapular plane or 45 degrees of abduction to minimize posterior stress.
- Internal Rotation: Gentle PROM to tolerance, avoiding aggressive posterior glide.
- Scapular Stability: Gentle isometric scapular exercises.
- Elbow/Wrist/Hand: Active ROM exercises to prevent stiffness.
Phase II: Early Motion and Gentle Strengthening (Weeks 6-12)
- Sling Discontinuation: Gradual weaning from sling as comfort and motion improve.
- Active-Assisted Range of Motion (AAROM): Progress to AAROM and then gentle Active Range of Motion (AROM) as tolerated.
- Isometric Strengthening: Initiation of pain-free isometric exercises for rotator cuff (infraspinatus, teres minor), deltoid, and scapular stabilizers.
- Light Resistance: Begin with light elastic band exercises for internal rotation and scapular retraction, avoiding positions of posterior apprehension.
- Proprioception: Wall slides, gentle weight shifts.
Phase III: Progressive Strengthening and Advanced Motion (Weeks 12-24)
- Full AROM: Aim for full pain-free range of motion.
- Progressive Strengthening: Increase resistance for rotator cuff and deltoid muscles. Introduce eccentric exercises.
- Functional Exercises: Incorporate exercises that mimic daily activities.
- Core Strengthening: Emphasize core stability and kinetic chain integration.
- Sport-Specific (if applicable): Begin low-level, sport-specific drills, ensuring proper form and control.
Phase IV: Return to Activity (Weeks 24+)
- Advanced Strengthening: Plyometric exercises, advanced proprioception, interval training.
- Sport-Specific Training: Gradually increase intensity and complexity of drills.
- Return to Play: Typically 6-9 months or longer for overhead athletes, depending on the severity of initial injury and repair, and only after achieving full strength, stability, and confidence, with a clearance from the surgeon and physical therapist.
Summary of Key Literature / Guidelines
The literature on the posterior shoulder approach and its associated pathologies is robust, reflecting a growing understanding of complex instability and reconstructive needs.
- Posterior Instability: Seminal work by authors like Hawkins, Matsen, and Burkhead has clarified the diagnosis and management of posterior glenohumeral instability. Current consensus emphasizes meticulous imaging (CT/MRI) for accurate diagnosis of labral tears, capsular defects, and bone loss. Arthroscopic techniques have advanced, but open posterior approaches remain critical for larger bone defects, challenging reductions, or specific reconstructive requirements.
-
Glenoid Bone Loss:
The management of posterior glenoid bone loss is a significant challenge. Studies by Provencher, Scheibel, and others highlight the importance of restoring glenoid anatomy, with various autograft (e.g., iliac crest) and allograft options being explored. The
Reverse Bankart Repair with Concomitant Glenoid Bone Augmentationis a recognized strategy for addressing significant posterior bone loss in recurrent instability. -
Reverse Hill-Sachs Lesions:
The concept of "engaging" reverse Hill-Sachs lesions driving instability is well-established. Procedures like
remplissage(infraspinatus tenodesis into the humeral head defect) have demonstrated success in preventing engagement and recurrence, particularly for smaller defects. Larger defects may necessitate osteochondral grafting or humeral head resurfacing. - Reverse Total Shoulder Arthroplasty (rTSA): While typically accessed anteriorly, the posterior approach can be critical in selected rTSA cases, especially for severe posterior glenoid bone loss or revision scenarios, allowing for optimal glenoid component positioning and screw fixation.
- Neurovascular Safety: Comprehensive anatomical studies continue to refine the understanding of axillary nerve trajectory and the safe zones for deltoid splitting. The 5 cm rule distal to the acromial angle is a widely accepted guideline.
Current guidelines underscore a personalized approach, integrating patient factors, injury characteristics, and surgeon experience. Future directions include further refinements in arthroscopic posterior stabilization techniques, biomaterials for labral and capsular reconstruction, and advancements in patient-specific instrumentation for glenoid augmentation. The ongoing dialogue in academic orthopedic surgery ensures that the "Precision Posterior Shoulder" approach remains a dynamic and evolving area of expertise.
Clinical & Radiographic Imaging