Surgical Anatomy: Approaches for Decompression of Leg Compartment Syndrome
Introduction & Epidemiology
Acute compartment syndrome (ACS) of the leg is a critical surgical emergency characterized by increased pressure within a confined osteofascial compartment, leading to impaired tissue perfusion, cellular ischemia, and eventual tissue necrosis. Left untreated, ACS can result in permanent functional deficits, including Volkmann's ischemic contracture, nerve palsy, limb loss, and systemic complications such as rhabdomyolysis and renal failure. Early diagnosis and emergent surgical decompression via fasciotomy are paramount to prevent irreversible damage.
The incidence of ACS of the leg is highest following high-energy trauma, particularly tibial shaft fractures, with rates reported between 1% and 9%. Other common etiologies include crush injuries, reperfusion injury after vascular repair, burns, arterial injury, prolonged limb compression, exertional injuries, and tight circumferential dressings or casts. While traumatic injuries are the most frequent cause, clinicians must maintain a high index of suspicion in any patient with a high-risk mechanism or presenting symptoms, irrespective of overt injury severity. Diagnosis relies primarily on clinical assessment, with intracompartmental pressure (ICP) measurements serving as an objective adjunct.
Surgical Anatomy & Biomechanics
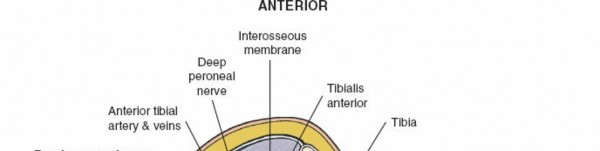
The leg is anatomically divided into four distinct osteofascial compartments by the tibia, fibula, interosseous membrane, and the unyielding deep crural fascia. Understanding the precise boundaries and contents of these compartments, as well as the proximity of neurovascular structures, is critical for effective and safe surgical decompression.
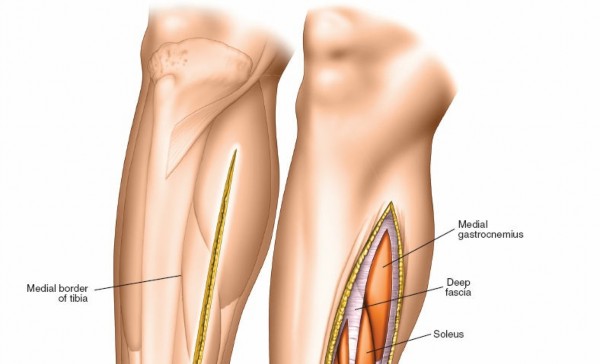
The tibia and fibula present distinct anatomical characteristics relevant to surgical approaches. The tibia possesses a large subcutaneous surface along its medial aspect, allowing for direct access to the bone. Conversely, the fibula is largely enveloped by muscle, becoming subcutaneous only at its proximal head and distal third, where it forms the lateral malleolus. Operations on most of the fibula therefore necessitate extensive muscle dissection. Furthermore, the tibia's primary neurovascular association is its nutrient artery, whereas the fibula is closely related to the common peroneal nerve and its branches, especially at the fibular neck.
The deep fascia of the leg is a tough, fibrous, and inelastic structure that encircles the calf muscles. It attaches firmly to the periosteum where the bones become subcutaneous. From its deep surface, two crucial intermuscular septa originate: the anterior intermuscular septum and the posterior intermuscular septum . Both septa extend to the fibula, effectively enclosing the peroneal, or lateral compartment , of the leg.
The four separate muscular compartments of the lower leg are:
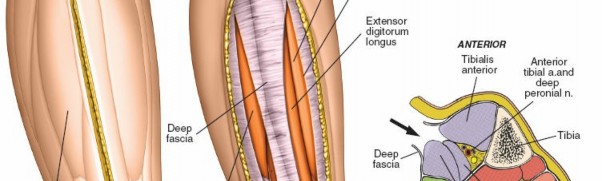
Anterior (Extensor) Compartment
This compartment lies between the tibia medially, the fibula and anterior intermuscular septum laterally, and the interosseous membrane posteriorly. Its roof is formed by the deep crural fascia.
*
Muscles:
Tibialis anterior, extensor hallucis longus (EHL), extensor digitorum longus (EDL), peroneus tertius.
*
Neurovascular Structures:
Deep peroneal nerve (motor innervation to compartment muscles, sensory to first web space), anterior tibial artery and accompanying veins. These structures lie on the interosseous membrane, between the tibialis anterior and EDL proximally, and then between the EHL and EDL distally.
*
Boundary:
Medial boundary is the lateral (extensor) surface of the tibia.
Lateral (Peroneal) Compartment
This compartment is located between the anterior and posterior intermuscular septa, lateral to the fibula.
*
Muscles:
Peroneus longus, peroneus brevis.
*
Neurovascular Structures:
Superficial peroneal nerve (motor to peroneal muscles, sensory to dorsum of foot, except first web space). This nerve courses between the peroneus longus and brevis and then pierces the deep fascia in the distal third of the leg, making it particularly vulnerable during fasciotomy.
*
Boundaries:
Anterior intermuscular septum anteriorly, posterior intermuscular septum posteriorly, fibula medially, deep crural fascia laterally.
Superficial Posterior Compartment
This is the largest compartment, lying posterior to the deep transverse fascia and the deep posterior compartment, and deep to the crural fascia.
*
Muscles:
Gastrocnemius, soleus, plantaris.
*
Neurovascular Structures:
Sural nerve (cutaneous sensory), sural arteries (branches of popliteal), branches of the tibial nerve to the calf muscles.
*
Boundaries:
Deep transverse fascia anteriorly, deep crural fascia posteriorly.
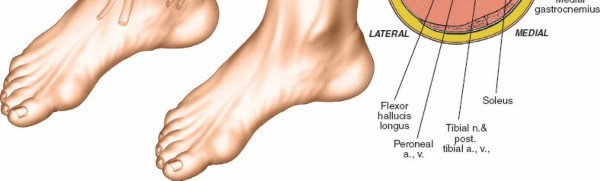
Deep Posterior Compartment
This compartment is situated anterior to the superficial posterior compartment, between the tibia, fibula, and interosseous membrane. It is covered by the deep transverse fascia.
*
Muscles:
Tibialis posterior, flexor digitorum longus (FDL), flexor hallucis longus (FHL).
*
Neurovascular Structures:
Tibial nerve, posterior tibial artery and veins, peroneal artery and veins. These neurovascular structures lie immediately superficial (posterior) to the deep transverse fascia, making their protection crucial during deep posterior compartment release.
*
Boundaries:
Tibia medially, fibula laterally, interosseous membrane anteriorly, deep transverse fascia posteriorly.
An appreciation of these compartmental boundaries and their contents is vital for surgical planning and execution. The figure below illustrates the cross-sectional anatomy of the leg compartments.
The deep fascia, by its unyielding nature, is the primary anatomical constraint contributing to the pathophysiology of compartment syndrome. The proximity of nerves, particularly the superficial peroneal nerve laterally and the tibial nerve and posterior tibial vessels posteromedially, necessitates meticulous surgical technique.
Further detailed understanding of the neurovascular bundles within the leg is essential. The anterior tibial artery and deep peroneal nerve are located within the anterior compartment, coursing on the interosseous membrane. The posterior tibial artery and tibial nerve descend within the deep posterior compartment, immediately superficial to the deep transverse fascia. The peroneal artery lies deep within the deep posterior compartment, closely associated with the fibula.
The image above provides a clear view of the neurovascular relationships within the deep posterior compartment.
Indications & Contraindications
The decision for fasciotomy is primarily a clinical one, requiring a high index of suspicion, particularly in high-risk patients with altered mental status or peripheral nerve blocks that mask symptoms. Objective ICP measurements serve as a valuable adjunct.
Indications for Fasciotomy
- Clinical Signs: The "6 Ps" – Pain out of proportion to injury (the most reliable early sign), Pallor , Paresthesia (nerve compression, early sign), Paralysis (late sign), Pulselessness (very late, ominous sign), and Poikilothermia . A tense, "wood-like" compartment upon palpation is a highly suggestive clinical finding.
-
Intracompartmental Pressure (ICP) Measurements:
- Absolute ICP > 30 mmHg (though thresholds can vary by institution and patient hemodynamics).
- Delta pressure (diastolic blood pressure - ICP) < 30 mmHg. This criterion accounts for the patient's mean arterial pressure and is often considered more reliable than an absolute pressure value alone, especially in hypotensive patients.
- Pressures that remain elevated or continue to rise over serial measurements.
- High-Risk Injuries with Clinical Suspicion: Tibial shaft fractures (especially high-energy or open fractures), crush injuries, prolonged limb ischemia (e.g., >6-8 hours), reperfusion injury following vascular repair, severe burns, electrical injuries, and prolonged immobilization on a hard surface.
-
Prophylactic Fasciotomy:
Considered in specific scenarios such as:
- Revascularization of an ischemic limb that has been ischemic for >4-6 hours.
- Combined arterial and venous injuries.
- High-energy tibial plateau or pilon fractures with significant soft tissue swelling or compromised vascularity.
- Patients with impaired consciousness where clinical monitoring is unreliable.
Contraindications for Fasciotomy
- Absence of Compartment Syndrome: Fasciotomy is an invasive procedure with potential complications; it should not be performed indiscriminately.
- Late Presentation with Irreversible Muscle Necrosis: In cases of delayed presentation (e.g., >12-24 hours) where muscle necrosis is clinically evident (rigidity, absent contractility, signs of established contracture), fasciotomy may not salvage viable tissue and could increase the risk of infection without functional benefit. In such scenarios, debridement of necrotic tissue or amputation may be more appropriate.
- Chronic Exertional Compartment Syndrome (CECS): While CECS may warrant fasciotomy, the indications and timing are elective and distinct from acute compartment syndrome. Acute fasciotomy is contraindicated for CECS.
The following table summarizes the key considerations for operative versus non-operative management of suspected compartment syndrome:
| Indication Type | Operative Fasciotomy | Non-Operative Management |
|---|---|---|
| Clinical | Classic 6 P's (Pain out of proportion, Pallor, Paresthesia, Paralysis, Pulselessness, Poikilothermia), Tense compartment | Mild swelling, pain responsive to analgesia, no neurologic deficit, palpable pulses |
| Pressure (ICP) | Absolute pressure >30 mmHg (or >20-25 mmHg in hypotensive patients) | ICP <30 mmHg, or Delta pressure (DBP-ICP) >30 mmHg |
| Delta pressure (DBP-ICP) <30 mmHg | Asymptomatic elevated pressure (e.g., from direct contusion, resolving) | |
| Associated Injury | Tibial shaft fracture, crush injury, prolonged ischemia, vascular repair, severe burns, electrical injury | Minor soft tissue trauma without significant compartment involvement |
| Timing | Acute onset, emergent intervention | Chronic exertional compartment syndrome (non-surgical if mild/responsive to rest/PT) |
| Special Cases | Prophylactic fasciotomy (e.g., prolonged limb ischemia, high-energy open tibial fractures) | Diagnostic uncertainty requiring serial examinations and ICP monitoring, resolution of symptoms with conservative measures (elevation, ice) |
Pre-Operative Planning & Patient Positioning
Once the decision for fasciotomy has been made, time is critical. Surgical decompression should ideally occur within 6 hours of symptom onset to maximize muscle viability and minimize long-term morbidity.
- Informed Consent: Despite the emergency, obtain informed consent, emphasizing the necessity of the procedure, potential complications (e.g., infection, nerve injury, chronic pain, scarring, need for skin grafting, reoperation), and the risk of limb loss if untreated.
- Anesthesia: General anesthesia is typically preferred to ensure patient immobility and comfort for a potentially prolonged procedure. Regional anesthesia may be used in conjunction but must not mask clinical signs post-operatively.
- Patient Positioning: The patient is positioned supine. The entire lower extremity from hip to toes must be prepped and draped in a sterile fashion, allowing full access to both the medial and lateral aspects of the leg. This enables the surgeon to perform either a single or two-incision approach and facilitate subsequent wound care and potential skin grafting. The knee should be slightly flexed.
- Tourniquet Application: A tourniquet may be applied to the proximal thigh, but it is typically not inflated if compartment syndrome is present or suspected, especially in cases of reperfusion injury, as inflation could exacerbate ischemia. If a fracture exists, the tourniquet may be helpful for initial hemostasis during the approach, but it should be released prior to fasciotomy if compartment syndrome is actively developing or diagnosed, to allow for assessment of compartment release and restoration of perfusion.
- Instrumentation: Ensure availability of a standard fasciotomy tray, electrosurgical cautery, negative pressure wound therapy (NPWT) dressings, and potentially skin grafting supplies.
- Imaging: Pre-operative X-rays of the leg are essential to identify any associated fractures.
Detailed Surgical Approach / Technique
The primary goal of fasciotomy is complete and rapid decompression of all affected compartments. The two-incision technique is widely considered the safest and most effective method for complete four-compartment decompression and is generally recommended.
General Principles for Fasciotomy
- Adequate Length: Incisions must be long enough to completely decompress the entire length of each compartment.
- Full Fascial Release: Each fascial layer must be incised along its entire length. Incomplete fasciotomy is a common cause of persistent compartment syndrome.
- Hemostasis: Achieve meticulous hemostasis to prevent hematoma formation, which can recreate a compartment syndrome or serve as a nidus for infection.
- Delayed Closure: The skin should not be closed primarily to prevent recurrent pressure buildup.
Two-Incision Technique (Four-Compartment Release)
This approach utilizes two longitudinal incisions – one anterolateral and one posteromedial – to access all four compartments.
1. Anterolateral Incision
This incision targets the anterior and lateral compartments.
*
Skin Incision:
Make a longitudinal incision, approximately 15-20 cm in length, centered over the fibula. It should extend from just distal to the fibular head to approximately 2-3 cm proximal to the lateral malleolus. This incision should be curvilinear, sweeping slightly anteriorly in the proximal leg and slightly posteriorly in the distal leg, to minimize scarring over bony prominences and facilitate later skin closure.
*
Deep Fascia Incision:
Incise the deep crural fascia along the full length of the skin incision. The underlying muscles of the anterior and lateral compartments will typically bulge.
*
Identifying Septa:
Identify the anterior intermuscular septum (located anterior to the fibula) and the posterior intermuscular septum (located posterior to the fibula).
*
Surgical Tip:
Palpate the fibula. The anterior septum will be just anterior to the fibula, and the posterior septum just posterior.
*
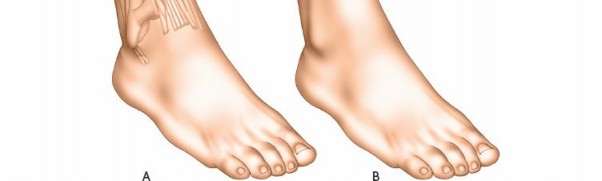
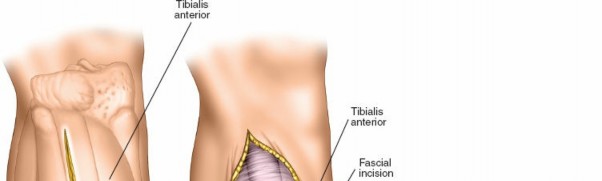
Anterior Compartment Release:
* Retract the anterior intermuscular septum and the lateral compartment muscles posteriorly.
* Incise the deep fascia directly overlying the anterior compartment. This incision should be medial to the anterior intermuscular septum and lateral to the tibia. Extend the fascial incision proximally and distally along the entire length of the compartment.
*
Neurovascular Consideration:
Be aware of the superficial peroneal nerve. It typically pierces the deep fascia in the distal third of the leg, anterior to the lateral malleolus. Proximally, it courses between the peroneus longus and extensor digitorum longus. Careful dissection in this region can help identify and protect it.
* Visually inspect for muscle bulging to ensure complete release.

The image above demonstrates the release of the anterior compartment.

Another view showcasing the anterior compartment release.
*
Lateral Compartment Release:
* Retract the anterior intermuscular septum and anterior compartment muscles anteriorly.
* Incise the deep fascia directly overlying the lateral compartment, located between the anterior and posterior intermuscular septa, lateral to the fibula. Extend this incision fully.
*
Neurovascular Consideration:
The superficial peroneal nerve courses within the lateral compartment. Careful identification and protection are crucial. It may be seen lying on the fibula or superficial to the peroneus brevis. Once identified, gently retract it to avoid injury.
* Visually inspect for muscle bulging to ensure complete release.
This image highlights the anatomical structures encountered during the lateral compartment release, with potential visualization of the superficial peroneal nerve.
2. Medial Incision
This incision targets the superficial and deep posterior compartments.

*
Skin Incision:
Make a longitudinal incision, approximately 15-20 cm in length, located about 2 cm posterior to the palpable posteromedial border of the tibia. This avoids the greater saphenous vein anteriorly and the sural nerve/small saphenous vein posteriorly. Extend it from just distal to the tibial tuberosity to approximately 2-3 cm proximal to the medial malleolus.
*
Deep Fascia Incision:
Incise the deep crural fascia along the full length of the skin incision. The gastrocnemius and soleus muscles (superficial posterior compartment) will bulge.
*
Superficial Posterior Compartment Release:
Directly incise the deep fascia overlying the gastrocnemius-soleus complex along its entire length.
*
Deep Posterior Compartment Release:
* Retract the gastrocnemius and soleus muscles posteriorly (medially). This exposes the deep transverse fascia.
*
Neurovascular Consideration:
Immediately superficial (posterior) to the deep transverse fascia lies the posterior tibial neurovascular bundle (posterior tibial artery, accompanying veins, and the tibial nerve). Carefully identify and protect this bundle.
* Incise the deep transverse fascia along its length. This can be done either anteriorly or posteriorly to the neurovascular bundle, but care must be taken to protect it. A common approach is to identify the tibial nerve and posterior tibial artery lying on the deep transverse fascia, gently retract them posteriorly, and then incise the deep transverse fascia.
* Extend this fascial incision proximally and distally. Proximally, ensure the soleus bridge (where soleus muscle fibers attach to the fibula) is released, as this can be a point of constriction. Distally, ensure the fascial attachments around the Achilles tendon are released.
* Visually inspect for muscle bulging of the tibialis posterior, FDL, and FHL to ensure complete release.

This image depicts the exposure of the deep posterior compartment after retraction of the superficial posterior muscles.

A close-up view demonstrating the incision of the deep transverse fascia.

This image clearly shows the neurovascular structures (tibial nerve and posterior tibial vessels) lying superficial to the deep transverse fascia, emphasizing the need for their protection.
Another perspective on the deep posterior compartment release, likely showing the muscle groups after decompression.
Single-Incision Techniques
While various single-incision approaches have been described (e.g., anterolateral or posteromedial), they are generally
less favored
for acute compartment syndrome requiring four-compartment release due to higher rates of incomplete decompression and increased risk to neurovascular structures.
*
Anterolateral Approach for Four Compartments:
This technically demanding approach involves subperiosteal elevation of the soleus from the fibula to access the deep posterior compartment. This carries a higher risk of injury to the peroneal artery, tibial nerve, and posterior tibial vessels.
*
Posteromedial Approach for Four Compartments:
Similarly challenging, requiring extensive dissection and retraction.
In cases where only specific compartments are involved (e.g., isolated anterior compartment syndrome, less common), a targeted single-incision approach might be considered, but caution is advised.
Wound Management After Fasciotomy
- Do Not Close Primarily: The skin incisions are left open due to significant tissue swelling. Attempting primary closure would recreate the compartment syndrome.
-
Temporary Wound Closure:
- Sterile Non-Adherent Dressings: Apply sterile, non-adherent dressings directly to the exposed muscle, followed by bulky sterile dressings.
- Negative Pressure Wound Therapy (NPWT): NPWT devices (e.g., vacuum-assisted closure) are frequently employed to manage exudate, promote granulation tissue formation, and gradually approximate wound edges.
- Vessel Loops / Shoelace Technique: Elastic vessel loops or sutures can be used to progressively approximate skin edges over several days to facilitate eventual delayed primary closure.
-
Second-Look Operation:
Typically performed within 24-48 hours. This allows for:
- Debridement: Removal of any necrotic or non-viable muscle tissue. Non-contractile, dark, or non-bleeding muscle should be debrided aggressively.
- Re-assessment: Confirm complete decompression and evaluate muscle viability.
- Wound Closure: Attempt delayed primary closure if swelling has significantly decreased. If skin tension is too high, serial approximation (shoelace technique) or split-thickness skin grafting (STSG) will be necessary. STSG is often required for larger defects or when delayed closure is not feasible.
Complications & Management
Despite prompt surgical intervention, fasciotomy is not without potential complications. Comprehensive understanding and proactive management are crucial for optimal patient outcomes.
| Complication | Incidence | Salvage Strategy |
|---|---|---|
| Infection | 5-20% | Aggressive serial debridement of necrotic tissue, appropriate broad-spectrum antibiotics, frequent wound care, negative pressure wound therapy (NPWT), delayed definitive closure (often requiring skin grafting). |
| Nerve Injury (Superficial Peroneal, Sural) | 10-20% (sensory deficits, particularly superficial peroneal) | Prevention is key by careful dissection. Post-operatively: observation for spontaneous recovery, neuropathic pain management, orthotics for motor deficits. For persistent motor deficits or severe painful neuromas, surgical exploration for neurolysis, nerve repair, or grafting may be considered, but is rare for sensory branches. |
| Persistent Compartment Syndrome | Rare (if adequate initial fasciotomy) | Immediate re-exploration, repeat full-length fasciotomy of all compartments, repeat intracompartmental pressure measurements, debridement of any newly identified necrotic tissue. Re-evaluation of the initial injury and any potential missed causes. |
| Volkmann's Ischemic Contracture | Variable (occurs if delayed or incomplete release) | Prevention is key by timely and complete fasciotomy. Established contracture management: intensive physical therapy, serial casting, surgical muscle release, tendon lengthening/transfer, neurolysis, or in severe cases, amputation. |
| Chronic Pain/Dysesthesia | Common (related to nerve irritation, scarring, or muscle damage) | Multimodal pain management (NSAIDs, neuropathic agents, physical therapy, desensitization techniques), scar massage, nerve blocks, psychological support. Surgical options (e.g., selective neurectomy) are rarely indicated. |
| Scarring/Cosmetic Deformity | High | Pressure garments, scar massage, silicone sheeting, camouflage makeup. Plastic surgery consultation for scar revision is rare in the acute phase but may be considered electively for functional or severe cosmetic concerns. |
| Skin Grafting/Delayed Wound Closure | Common (for large defects or persistent swelling) | Split-thickness skin grafting (STSG) or full-thickness skin grafting. NPWT to prepare wound bed. Progressive wound approximation techniques (e.g., vessel loops, external fixator-assisted closure). |
| Rhabdomyolysis/Renal Failure | Variable (depends on initial insult severity, often from crush injury) | Aggressive intravenous fluid resuscitation, urine alkalinization (bicarbonate infusion), monitoring of renal function, serum creatine kinase (CK), electrolytes. Dialysis may be required in severe cases. |
| Edema/Swelling | Common | Elevation of the limb, compression stockings, early mobilization, physical therapy to reduce swelling and improve lymphatic drainage. |
| Deep Venous Thrombosis (DVT) | Variable | Prophylactic anticoagulation as appropriate, early mobilization. Management of established DVT includes therapeutic anticoagulation. |
Post-Operative Rehabilitation Protocols
Post-fasciotomy rehabilitation is a critical component of functional recovery. Protocols must be individualized based on the extent of muscle damage, presence of associated injuries (e.g., fractures), and wound status.
Acute Phase (0-2 weeks)
- Wound Management: Meticulous wound care, including dressing changes, management of NPWT, and preparation for delayed closure or skin grafting. Keep the leg elevated to minimize edema.
- Range of Motion (ROM): Initiate gentle, passive and active-assisted range of motion exercises for the ankle and toes as soon as surgical stability allows and without compromising wound integrity. Avoid extreme plantarflexion or dorsiflexion if soft tissue repairs are tenuous.
- Pain Management: Administer appropriate analgesia to facilitate early movement and comfort.
- Weight-Bearing Status: Non-weight-bearing or touch-down weight-bearing on the affected limb until wounds are stable and any associated fractures demonstrate early healing. Progress to weight-bearing as tolerated once wound closure is achieved and deemed safe.
Subacute Phase (2-6 weeks)
- Wound/Scar Management: Continue wound care. Once wounds are closed, begin scar massage, desensitization techniques for nerve irritation, and consider silicone sheeting or pressure garments to minimize hypertrophic scarring.
- Progressive ROM: Advance ankle and foot ROM exercises, including active and passive stretching. Address any developing contractures early.
- Strengthening: Initiate isometric strengthening exercises for all leg muscle groups. Gradually progress to isotonic exercises with light resistance, focusing on both concentric and eccentric contractions.
- Gait Training: Once partial weight-bearing is initiated, begin gait training with appropriate assistive devices (crutches, walker). Focus on proper biomechanics and symmetry.
- Neuromuscular Re-education: Address any balance or proprioceptive deficits resulting from nerve injury or prolonged immobilization.
Reconstructive/Advanced Phase (6 weeks - 6 months and beyond)
- Intensive Physical Therapy: Continue a comprehensive exercise program focusing on strength, endurance, flexibility, balance, and proprioception.
- Functional Training: Incorporate sport-specific or activity-specific drills for patients aiming to return to higher-level activities.
- Addressing Deficits: Manage persistent deficits such as muscle weakness, foot drop (requiring an ankle-foot orthosis, AFO), or chronic pain.
-
Secondary Procedures:
Evaluate for the need for secondary surgical interventions such as:
- Tendon Lengthening/Transfer: For fixed contractures (e.g., Achilles lengthening for equinus deformity) or to address muscle imbalance/weakness.
- Scar Revision: For significant cosmetic or functional issues.
- Nerve Exploration/Neurolysis: Rarely indicated for intractable neuropathic pain or motor deficits.
- Long-Term Monitoring: Patients should be followed for potential late complications such as chronic pain, nerve dysfunction, and functional limitations.
Summary of Key Literature / Guidelines
The management of acute compartment syndrome is a well-established area in orthopedic surgery, with key principles largely consistent across major guidelines and literature.
- Time is Muscle: The overwhelming consensus is that early diagnosis and emergent surgical decompression are critical. Delay in fasciotomy beyond 6-8 hours significantly increases the risk of irreversible muscle necrosis, nerve damage, and long-term functional impairment. Studies by McQueen and Court-Brown, among others, have highlighted the strong correlation between time to fasciotomy and patient outcome.
- Clinical Diagnosis Remains Primary: While intracompartmental pressure measurements are valuable objective adjuncts, the diagnosis of ACS is primarily clinical. A high index of suspicion, particularly in high-risk patients or those with impaired consciousness, is paramount. The "pain out of proportion" symptom is consistently identified as the earliest and most reliable indicator.
- ICP Measurement Thresholds: While absolute ICP values (e.g., >30 mmHg) are often cited, the delta pressure (diastolic blood pressure - ICP < 30 mmHg) is considered by many to be a more physiologically accurate threshold, as it accounts for the patient's individual blood pressure and perfusion status. Matsen et al.'s work contributed significantly to the understanding of critical pressure differentials.
- Complete Four-Compartment Release: The two-incision technique for complete decompression of all four leg compartments (anterior, lateral, superficial posterior, deep posterior) is the gold standard approach. It allows for thorough fascial release and minimizes the risk of incomplete decompression, which is a leading cause of persistent compartment syndrome and poor outcomes. Single-incision techniques are generally considered insufficient for comprehensive release of all four compartments in acute settings and carry higher risks.
- Delayed Wound Closure: Leaving the fasciotomy wounds open and performing delayed primary closure or skin grafting at a second-look operation (typically 24-48 hours later) is standard practice. This prevents recurrent pressure and allows for debridement of any necrotic tissue. Negative pressure wound therapy has become a valuable tool in managing these open wounds, promoting granulation, and facilitating eventual closure.
- Prevention and Management of Complications: Awareness of potential complications, particularly nerve injury (superficial peroneal nerve being most vulnerable), infection, and chronic pain, guides surgical technique and post-operative care. Proactive strategies, such as meticulous dissection, appropriate antibiotic prophylaxis, and early rehabilitation, are emphasized.
- Chronic Exertional Compartment Syndrome (CECS): It is important to differentiate acute CS from CECS. While CECS may also be treated with fasciotomy, it is an elective procedure performed for activity-related pain, and its indications and surgical approach often differ from acute emergent fasciotomy.
In conclusion, a thorough understanding of leg surgical anatomy, prompt clinical diagnosis, judicious use of ICP measurements, and adherence to established surgical principles for complete and safe fasciotomy are essential for managing acute leg compartment syndrome effectively and optimizing patient recovery.
Clinical & Radiographic Imaging

