Unlocking the Anatomy of the Dorsal Approach to the Wrist
Introduction & Epidemiology
The dorsal approach to the wrist is a fundamental surgical pathway providing direct access to the posterior aspects of the distal radius, carpal bones, and the associated ligamentous and tendinous structures. This approach is indispensable for managing a diverse range of pathologies, including distal radius fractures, carpal fractures (e.g., scaphoid non-unions), dorsal wrist ganglion excisions, radioscapholunate ligamentous repair or reconstruction, synovectomies, and dorsal wrist arthrodeses. Its historical roots trace back to early descriptions of wrist anatomy and the evolution of surgical techniques for fracture fixation and soft tissue management.
Epidemiologically, wrist pathologies requiring a dorsal approach are common. Distal radius fractures, particularly those with dorsal comminution or articular involvement, represent a significant proportion of orthopedic trauma. Scaphoid non-unions, often necessitating dorsal grafting and fixation, are also frequent, with reported non-union rates varying but presenting a considerable clinical challenge. Dorsal wrist ganglions are among the most common soft tissue masses of the hand and wrist, with surgical excision often pursued for symptomatic relief or cosmetic reasons. Conditions such as rheumatoid arthritis frequently involve dorsal wrist synovitis, requiring surgical debridement via this exposure. Understanding the intricate dorsal anatomy is paramount for safe and effective surgical intervention, minimizing iatrogenic injury, and optimizing patient outcomes.
Surgical Anatomy & Biomechanics
The dorsal aspect of the wrist is a complex region comprising an intricate arrangement of tendons, retinacular structures, neurovascular elements, and bony and ligamentous components. A thorough understanding of these relationships is critical for successful dorsal wrist surgery.
Extensor Compartments and Retinaculum
Twelve tendons traverse the dorsal wrist, organized into six distinct fibrous compartments beneath the extensor retinaculum. The extensor retinaculum, a robust thickening of the deep forearm fascia, originates from the lateral margin of the radius and inserts into the pisiform and triquetrum medially. Its primary biomechanical function is to prevent bowstringing of the extensor tendons during wrist motion, maintaining their mechanical advantage. Fibrous septa extend from the deep surface of the retinaculum to the underlying periosteum of the distal radius and ulna, creating the six osteofascial tunnels. These septa must be meticulously identified and separated from the retinaculum during surgical exposure to allow individual compartment opening and tendon mobilization.
The contents of the six extensor compartments, from radial to ulnar, are:
- First Compartment: Abductor Pollicis Longus (APL) and Extensor Pollicis Brevis (EPB). This compartment is located radial to the radial styloid.
- Second Compartment: Extensor Carpi Radialis Longus (ECRL) and Extensor Carpi Radialis Brevis (ECRB). These tendons pass over Lister's tubercle.
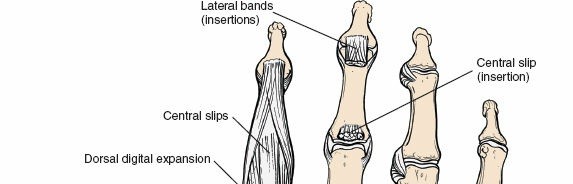
- Third Compartment: Extensor Pollicis Longus (EPL). This tendon hooks around Lister's tubercle, changing its direction.
- Fourth Compartment: Extensor Digitorum Communis (EDC) and Extensor Indicis Proprius (EIP). This is typically the largest compartment, positioned over the lunate.
- Fifth Compartment: Extensor Digiti Minimi (EDM). This compartment lies ulnar to the distal radioulnar joint (DRUJ).
- Sixth Compartment: Extensor Carpi Ulnaris (ECU). This tendon is contained within a fibro-osseous tunnel along the ulnar styloid.

Figure 5-11 (conceptual representation): Transverse section of the dorsal wrist demonstrating the extensor retinaculum and its six fibrous compartments with their respective tendon contents.
Neurovascular Structures
Several critical neurovascular structures are at risk during a dorsal approach:
- Superficial Radial Nerve (SRN): This sensory nerve emerges from beneath the brachioradialis tendon approximately 7-9 cm proximal to the radial styloid and then divides into multiple branches that innervate the dorsum of the thumb, index, middle, and radial aspect of the ring finger. It is highly susceptible to iatrogenic injury, traction neuropraxia, or entrapment within scar tissue, leading to persistent paresthesias or painful neuromas.
- Dorsal Cutaneous Branch of the Ulnar Nerve: This sensory nerve typically emerges about 5-6 cm proximal to the ulnar styloid, passing dorsally over the distal ulna to innervate the dorsum of the medial hand and fifth finger. It is less commonly injured with radial-sided dorsal approaches but is at risk during ulnar-sided dissections or wide exposures.
- Posterior Interosseous Nerve (PIN): As the terminal motor branch of the deep radial nerve, the PIN courses through the fourth extensor compartment. After innervating the posterior forearm muscles, it terminates in a sensory articular branch supplying the dorsal wrist capsule. In certain procedures (e.g., dorsal wrist denervation for chronic pain), this nerve is intentionally resected. Care must be taken to avoid unintended injury during deeper dissections of the joint capsule.
- Dorsal Venous Network: A prominent superficial venous network covers the dorsal wrist and hand. Meticulous dissection and careful retraction are necessary to preserve these veins, minimizing post-operative edema and improving wound healing.
Bony Anatomy and Ligamentous Structures
Landmarks:
Two primary bony landmarks define the dorsal wrist:
-
Radial Styloid Process:
This is the distal-most projection of the lateral radius. It serves as the attachment site for the brachioradialis tendon and articulates medially with the scaphoid. Its critical position means that strong and sudden radial deviation can cause impaction of the scaphoid against the radial styloid, potentially leading to a scaphoid fracture or a radial styloid fracture. The radial styloid is sometimes resected in cases of scaphoid non-union with impingement or advanced radioscaphoid arthrosis to decompress the joint and improve range of motion.

Figure 5-14A (conceptual representation): Illustrates the articulation between the radial styloid and the scaphoid bone. Figure 5-14B (conceptual representation): Depicts the mechanism of scaphoid or radial styloid fracture due to forceful radial deviation and impaction. -
Lister's Tubercle:
A dorsal tubercle on the distal radius, it acts as a pulley for the EPL tendon, redirecting its course towards the thumb. It is a key landmark for orienting dorsal incisions and identifying the third extensor compartment.

Figure 5-13 (conceptual representation): Highlights Lister's tubercle on the dorsal aspect of the distal radius, serving as a palpable landmark.
Distal Radius:
The dorsal aspect of the distal radius includes the dorsal rim, the dorsal lunate facet, and the sigmoid notch for articulation with the ulna. Understanding the inclination and angulation of the dorsal radius is vital for fracture reduction and plate positioning.
Carpal Bones:
The dorsal carpal bones—scaphoid, lunate, triquetrum, and the distal carpal row—are the primary targets for many dorsal procedures.
*
Scaphoid:
Its proximal pole is accessible dorsally, crucial for non-union repair and bone grafting.
*
Lunate:
Centrally located, it's often the focus for dorsal capsulotomy, synovectomy, or four-corner arthrodesis.
*
Triquetrum:
Lies ulnar to the lunate.

Figure 5-15 (conceptual representation): Dorsal view of the carpal bones, illustrating their relationships and relative positions, particularly the scaphoid, lunate, and triquetrum.
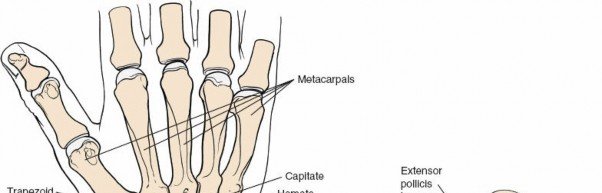
Figure 5-16 (conceptual representation): Closer anatomical view showing the dorsal surfaces of the proximal carpal row and their articulations.
Ligamentous Anatomy:
The dorsal wrist capsule is reinforced by several key ligaments:
*
Dorsal Radiocarpal Ligament (DRCL):
The primary dorsal stabilizer of the wrist, running from the distal radius to the triquetrum.
*
Scapholunate Ligament (SLL) and Lunotriquetral Ligament (LTL):
Intrinsic ligaments vital for carpal stability. Dorsal capsulotomy must be performed carefully to avoid or strategically address these structures, particularly in cases of instability.
Biomechanics:
The dorsal approach inherently involves manipulation of the retinaculum and often the capsule, which can impact wrist biomechanics.
*
Retinacular release:
While necessary for exposure, it risks tendon bowstringing if not adequately repaired or reconstructed. This can alter moment arms and reduce tendon efficiency.
*
Capsulotomy:
Extensive capsular incisions can destabilize the carpus, emphasizing the need for meticulous repair where feasible.
*
Plate Fixation:
Dorsal plating for distal radius fractures can contribute to EPL tendon irritation or rupture, especially with plate prominence or inadequate soft tissue coverage. Plate design and positioning are critical considerations.
Indications & Contraindications
The dorsal approach to the wrist is versatile but not universally applicable. Careful patient selection and pre-operative planning are paramount.
Indications
Operative Indications (Requiring Dorsal Approach):
-
Distal Radius Fractures:
- Dorsal comminution or displacement requiring direct reduction and dorsal plate fixation.
- Articular step-off or gap requiring direct visualization for reduction.
- Revision surgery for failed volar plating (e.g., dorsal malunion).
-
Carpal Fractures and Non-unions:
- Scaphoid fractures (e.g., proximal pole fractures, non-unions) requiring vascularized or non-vascularized bone grafting and fixation.
- Non-unions of other carpal bones accessible dorsally.
- Dorsal Wrist Ganglion Excision: The most common soft tissue mass on the dorsum of the wrist, arising from the scapholunate ligament.
-
Dorsal Wrist Arthrodesis:
- Four-corner (radioscapholunate, scaphotrapeziotrapezoid) arthrodesis for painful degenerative conditions (e.g., SLAC, SNAC wrist).
- Total wrist arthrodesis for severe pan-carpal arthritis or instability.
-
Synovectomy:
- Chronic synovitis (e.g., rheumatoid arthritis) involving the dorsal wrist.
-
Ligamentous Repair/Reconstruction:
- Dorsal scapholunate ligament repair or reconstruction (e.g., capsulodesis, tendon graft).
- Other dorsal carpal ligament instabilities.
- Excision of Carpal Boss: Painful osteophyte at the carpometacarpal joint.
- De Quervain's Tenosynovitis Release: Surgical decompression of the first dorsal compartment.
- Posterior Interosseous Nerve Neurectomy: For chronic, diffuse dorsal wrist pain.
- Tendon Transfers: For wrist or finger extension deficiencies.
Contraindications
- Active Infection: Cellulitis, abscess, or osteomyelitis in the surgical field.
- Severe Dorsal Soft Tissue Compromise: Extensive scarring from previous surgeries, severe open wounds, or burns that would compromise wound healing.
- Vascular Insufficiency: Pre-existing conditions compromising distal perfusion.
- Primary Volar Pathology: Where a volar approach provides superior access and less morbidity (e.g., most volar-displaced distal radius fractures, carpal tunnel release).
- Uncontrolled Medical Comorbidities: Increasing anesthetic or surgical risk.
- Poor Patient Compliance: Unwillingness or inability to adhere to post-operative rehabilitation protocols.
Table: Operative vs. Non-Operative Indications for Dorsal Wrist Pathology
| Pathology Type | Operative Indication (Dorsal Approach) | Non-Operative Indication |
|---|---|---|
| Distal Radius Fracture | Unstable dorsal comminution, significant articular step-off/gap, dorsal malunion requiring revision | Minimally displaced/stable fractures, adequate reduction with cast/splint |
| Scaphoid Fracture/Non-union | Proximal pole fracture, established non-union with displacement/humpback deformity, avascular necrosis | Acute, stable, non-displaced fractures managed with casting; asymptomatic non-unions |
| Dorsal Wrist Ganglion | Symptomatic (pain, weakness, nerve compression), recurrent after aspiration, cosmetic concern | Asymptomatic, small, first presentation (often managed with aspiration) |
| Wrist Arthritis/Instability | Symptomatic advanced arthritis (SLAC/SNAC), painful instability not responding to conservative care | Mild symptoms, early stages, amenable to splinting, NSAIDs, injections, activity modification |
| Tenosynovitis (e.g., De Quervain's) | Persistent symptoms despite conservative management, functional impairment | Acute phase, mild symptoms, amenable to splinting, NSAIDs, injections |
| Synovitis (e.g., RA) | Persistent inflammatory synovitis despite medical management, impending tendon rupture | Early synovitis, controlled with systemic therapy, no functional impairment |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for anticipating anatomical variations, identifying specific pathology, and optimizing surgical execution.
Pre-operative Imaging
- Standard Radiographs: Anteroposterior (AP), lateral, and oblique views are crucial for assessing bony architecture, fracture patterns, carpal alignment, and arthritic changes. Dedicated scaphoid views are necessary for suspected scaphoid pathology.
- Computed Tomography (CT) Scan: Indispensable for detailed assessment of fracture complexity, articular involvement (e.g., distal radius, scaphoid), non-union characteristics, and pre-operative templating for hardware. Provides excellent bony detail.
- Magnetic Resonance Imaging (MRI): Valuable for evaluating soft tissue pathology, ligamentous injuries (e.g., scapholunate or lunotriquetral tears), avascular necrosis (e.g., scaphoid, lunate), and inflammatory conditions (e.g., synovitis).
- Arthrography: Occasionally used in conjunction with MRI or CT to delineate ligamentous injuries.
Anesthesia
Regional anesthesia (e.g., axillary or supraclavicular block) combined with monitored anesthesia care or general anesthesia is typically preferred. A regional block provides excellent post-operative pain control and muscle relaxation, which can facilitate tissue handling.
Tourniquet
A pneumatic tourniquet placed on the upper arm is routinely used to provide a bloodless surgical field, enhancing visualization and precision. Tourniquet time should be monitored.
Patient Positioning
- Supine Position: The patient is placed supine on the operating table.
- Arm Board/Hand Table: The affected arm is positioned on a dedicated hand table, allowing for full range of motion of the wrist and fingers, and ensuring unimpeded access for the surgical team. The hand table should be securely affixed and padded.
- Forearm Position: The forearm is typically pronated to present the dorsal aspect of the wrist. Slight wrist flexion or extension may be employed depending on the specific area requiring maximal exposure.
- Traction (Optional): For certain procedures, such as fracture reduction or carpal instability assessment, sterile finger traps with longitudinal traction may be applied to distract the joint, aiding visualization and reduction. This requires an appropriately positioned outrigger on the hand table.
Sterilization and Prophylaxis
- Antibiotic Prophylaxis: Standard broad-spectrum prophylactic antibiotics are administered intravenously within 60 minutes prior to incision, following institutional protocols.
- Skin Preparation: The entire arm, from mid-humerus to fingertips, is prepped with an antiseptic solution (e.g., chlorhexidine or povidone-iodine based solution) and allowed to dry.
- Draping: Standard sterile draping is applied, ensuring adequate exposure of the surgical field while maintaining sterility.
Detailed Surgical Approach / Technique
The dorsal approach necessitates a systematic, layered dissection to minimize trauma to vital structures and optimize exposure for specific pathologies.
1. Incision Planning and Skin Incision
The choice of skin incision depends on the specific pathology and desired exposure.
*
Straight Longitudinal Incision:
Most commonly employed, centered over Lister's tubercle, extending proximally and distally as needed. This provides direct access but can risk injury to superficial radial nerve branches laterally and dorsal cutaneous ulnar nerve branches medially.
*
Curvilinear or S-shaped Incision:
May be used to improve cosmesis and potentially reduce tension on the skin edges, particularly for longer exposures.
*
Transverse Incision:
Less commonly used for deep access but may be suitable for small, localized lesions like a dorsal ganglion excision.
*
Zigzag or Wavy Incision:
Primarily for addressing specific structures like ganglions over the scapholunate area.
Landmark Identification:
Prior to incision, palpate and mark the radial styloid, ulnar styloid, Lister's tubercle, and the extensor tendon compartments.

Figure 5-12 (conceptual representation): Illustrates common dorsal wrist incision lines, including straight longitudinal, curvilinear, and transverse options, typically centered around key bony landmarks.
2. Skin and Subcutaneous Dissection
- The incision is made through the skin with a sharp scalpel.
- Subcutaneous tissue is carefully dissected using fine scissors or a scalpel, proceeding directly to the deep fascia.
-
Nerve Protection:
Meticulous dissection is crucial to identify and protect branches of the superficial radial nerve (radially) and the dorsal cutaneous branch of the ulnar nerve (ularly). These nerves are highly variable in their course but generally lie within the subcutaneous fat. Blunt dissection or spreading with small curved scissors parallel to the nerve's course can help identify them. Gentle retraction with small hooks or vessel loops is preferred over aggressive retraction. The dorsal venous network should also be preserved where possible to reduce post-operative edema.

Figure 5-18 (conceptual representation): Shows the initial skin and subcutaneous dissection, highlighting the superficial neurovascular structures that must be protected.
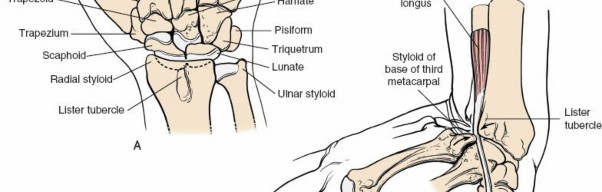
Figure 5-19 (conceptual representation): Close-up illustrating careful blunt dissection to identify and protect the superficial radial nerve branches.
3. Extensor Retinaculum Incision and Compartment Exposure
Once the deep fascia overlying the extensor retinaculum is exposed, the retinaculum itself is carefully incised.
*
Standard Incision:
For general dorsal wrist exposure (e.g., dorsal radius fracture, arthrodesis), the retinaculum is typically incised longitudinally along the ulnar border of the third extensor compartment (EPL). This allows the third compartment (EPL) to be retracted radially, and compartments four, five, and six to be retracted ulnarly, or vice versa. The retinaculum can then be reflected radial and ulnar, preserving its continuity for later repair.

Figure 5-20 (conceptual representation): Depicts the longitudinal incision of the extensor retinaculum, typically along the ulnar border of the third compartment.
*
Specific Compartment Opening:
For targeted procedures like De Quervain's release, only the first compartment is opened. For synovectomy or ganglion excision, the fourth compartment interval is often used.
*
Identification of Compartments:
After incision, carefully identify the fibrous septa separating the compartments. These septa are released from the deep surface of the retinaculum, allowing the individual tendon compartments to be fully opened and their contents to be mobilized and retracted.

Figure 5-21 (conceptual representation): Demonstrates the opened retinaculum, exposing the underlying extensor tendons within their respective compartments.

Figure 5-22 (conceptual representation): Shows individual extensor compartments after septa release, allowing for mobilization of the tendon bundles.
*
Tendon Management:
The tendons within the desired compartments (often the EDC/EIP in the fourth compartment) are gently retracted, typically ulnarly or radially depending on the target area, to expose the underlying dorsal wrist capsule. The EPL tendon (third compartment) is often retracted radially.

Figure 5-23 (conceptual representation): Identifies the specific extensor tendons after exposure, prior to deeper dissection.
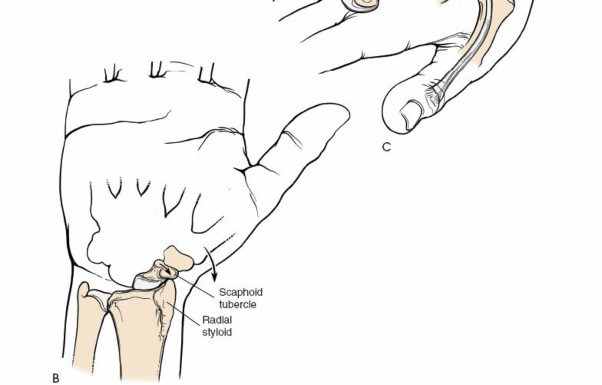
Figure 5-24 (conceptual representation): Further dissection and retraction of the extensor tendons to expose the dorsal wrist capsule.
4. Dorsal Wrist Capsulotomy and Joint Exposure
- The dorsal wrist capsule is a dense fibrous layer overlying the carpal bones and distal radius. The choice of capsulotomy incision depends on the specific surgical goal.
- Longitudinal Incision: A straight longitudinal incision through the capsule, often in the interval between the third and fourth compartments or the fourth and fifth, provides access to the central carpus (lunate, capitate).
- H-shaped or U-shaped Incision: These incisions are commonly used for wider exposure, such as for four-corner arthrodesis or extensive synovectomy. A common approach involves creating a distally based "U" or "H" flap, which can be repaired later. The capsulotomy can also be made between the third and fourth compartments and extended proximally and distally as required.
-
Ligament Protection:
Care must be taken to avoid or strategically address intrinsic carpal ligaments (e.g., scapholunate, lunotriquetral) unless the procedure specifically targets them. The dorsal radiocarpal ligament is often part of the capsular flap.

Figure 5-25 (conceptual representation): Shows the dorsal wrist capsule after tendon retraction, illustrating potential sites for capsulotomy.
5. Specific Procedures (Examples)
- Distal Radius Fracture Fixation: Once the joint is exposed, fracture fragments are directly visualized. Ligamentotaxis or direct manipulation is used for reduction. Plate and screw fixation is then applied to achieve stable anatomical reduction. Dorsal plates are typically low-profile to minimize tendon irritation.
- Scaphoid Non-union Repair: The non-union site is débrided, sclerotic bone is removed, and a bone graft (autograft or allograft) is packed into the defect. Fixation with headless compression screws or K-wires is then performed. Access can be tailored depending on the fracture location (e.g., radial approach for waist, dorsal for proximal pole).
- Dorsal Wrist Arthrodesis: For a four-corner fusion, cartilage is resected from the radioscaphoid, radiolunate, capitolunate, and triquetrohamate joints. Bone graft is packed into the decorticated joint spaces, and a dorsal plate (e.g., PRC plate) is applied for stable fixation.
6. Wound Closure
- Capsule Repair: If an H-shaped or U-shaped capsulotomy was performed, the capsular flap is meticulously repaired using absorbable sutures. This helps restore carpal stability and provides a barrier for underlying structures.
- Retinaculum Repair: The extensor retinaculum is repaired to prevent tendon bowstringing. However, it is often repaired loosely or partially, especially if significant edema is anticipated or if there's a risk of creating pressure on tendons (e.g., after dorsal plating). Sometimes, a local flap of retinaculum is used to cover hardware, or a portion may be excised if no bowstringing is expected (e.g., first compartment release).
- Subcutaneous Tissue: The subcutaneous layer is closed with absorbable sutures to obliterate dead space and reduce tension on the skin.
- Skin Closure: The skin is closed with staples, non-absorbable sutures, or absorbable sutures, ensuring good apposition of the wound edges.
- Dressing: A sterile, non-adherent dressing is applied, followed by appropriate immobilization (splint or cast) based on the procedure performed.
Complications & Management
Despite meticulous technique, complications can occur after a dorsal wrist approach. Anticipation and prompt management are crucial for optimal outcomes.
Common Complications
-
Nerve Injury:
- Superficial Radial Nerve (SRN): Incidence of injury or irritation ranges from 5% to 20%. Can lead to persistent paresthesias, dysesthesias, or painful neuroma formation.
- Dorsal Cutaneous Branch of Ulnar Nerve: Less common, but can result in sensory deficits on the ulnar dorsum.
- Posterior Interosseous Nerve (PIN): Intentional resection for denervation is common, but unintended motor branch injury is rare.
-
Tendon Complications:
- Adhesions/Tenosynovitis: Scarring around tendons or within compartments can limit gliding and cause pain or stiffness.
- Tendon Rupture: Most commonly, the Extensor Pollicis Longus (EPL) tendon can rupture, particularly after dorsal plating of distal radius fractures due to irritation or compromise of blood supply. Other extensor tendons are less commonly affected.
- Bowstringing: If the extensor retinaculum is inadequately repaired or excessively released, tendons may bowstring, leading to reduced mechanical advantage and weakness.
- Infection: Superficial or deep wound infection, requiring antibiotics, debridement, or implant removal.
- Vascular Injury: Rare due to the predominantly tendinous and bony nature of the dorsal wrist, but small dorsal vessels may be injured, leading to hematoma.
- Joint Stiffness/Arthrosis: Post-operative immobilization and scar tissue can contribute to restricted wrist motion.
- Non-union/Malunion: Particularly relevant in fracture fixation or arthrodesis procedures.
- Hardware Issues: Plate or screw prominence causing tendon irritation, skin irritation, or pain; hardware failure (rare).
- Persistent Pain: Chronic dorsal wrist pain, which may be multifactorial (e.g., subtle instability, nerve irritation, complex regional pain syndrome).
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Estimated Incidence | Salvage Strategies |
|---|---|---|
| Superficial Radial Nerve Neuroma/Neuritis | 5-20% | Conservative (NSAIDs, splinting, nerve blocks, desensitization); surgical (neurolysis, neuroma excision with/without nerve graft, targeted muscle reinnervation) |
| EPL Tendon Rupture | 1-3% (post-DRF plating) | Tendon transfer (e.g., EIP to EPL) is the primary treatment. |
| Tendon Adhesions/Tenosynovitis | Variable | Hand therapy (gliding exercises, scar massage); NSAIDs; corticosteroid injections; surgical tenolysis in refractory cases. |
| Infection (Superficial/Deep) | 1-5% | Superficial: Oral antibiotics, local wound care. Deep: IV antibiotics, surgical irrigation & debridement, hardware removal (if stable union achieved or in chronic cases), possible negative pressure wound therapy. |
| Wrist Stiffness/ROM Loss | Variable | Aggressive hand therapy (active/passive ROM, stretching); dynamic/static progressive splinting; surgical capsulolysis in severe, recalcitrant cases. |
| Non-union (Fracture/Arthrodesis) | Variable | Revision surgery with débridement, bone grafting, and rigid internal fixation; biological augmentation (e.g., PRP, bone marrow aspirate). |
| Hardware Prominence/Irritation | 5-10% | Hardware removal after bone healing/fusion is complete; soft tissue interposition for unavoidable plate contact. |
| CRPS (Complex Regional Pain Syndrome) | <1% | Multidisciplinary approach: pain management (nerve blocks, neuromodulators), intensive hand therapy, psychological support. Early diagnosis and treatment are critical. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to maximizing functional recovery and minimizing complications after a dorsal wrist approach. Protocols vary based on the specific procedure, patient factors, and surgeon preference.
1. Immobilization Phase (Acute Phase)
- Duration: Typically 2-6 weeks, depending on the stability achieved surgically.
-
Type of Immobilization:
- Splint: Removable custom-molded thermoplastic splint (sugar-tong, dorsal block, or volar wrist splint) allows for wound inspection and hygiene.
- Cast: Short arm cast or long arm cast (e.g., for unstable fractures, early scaphoid non-unions) for more rigid immobilization.
- Goals: Protect the surgical repair/fixation, manage pain and swelling, promote wound healing.
-
Activities:
- Elevation to minimize edema.
- Finger active range of motion (AROM) exercises (flexion/extension, abduction/adduction) to prevent stiffness and maintain digital function.
- Elbow and shoulder AROM exercises.
- Avoidance of weight-bearing or forceful gripping.
2. Early Mobilization Phase (Subacute Phase)
- Initiation: Typically 2-6 weeks post-operatively, after initial healing and stability are confirmed (e.g., radiographic union for fractures).
- Goals: Restore pain-free wrist range of motion, prevent adhesions, improve tendon gliding.
-
Activities (guided by hand therapist):
- Passive Range of Motion (PROM): Gentle, controlled wrist flexion/extension, radial/ulnar deviation.
- Active Range of Motion (AROM): Assisted and unassisted wrist movements.
- Tendon Gliding Exercises: Specific exercises to promote differential gliding of extensor tendons.
- Scar Management: Gentle massage, silicone sheeting, or other modalities to minimize scar tissue formation and adhesion.
- Light Gripping: Introduction of very light grip strengthening exercises (e.g., squeezing soft foam).
3. Strengthening Phase (Intermediate Phase)
- Initiation: Typically 6-12 weeks post-operatively, once pain is well-controlled and a good range of motion is established.
- Goals: Progressive strengthening of wrist and forearm musculature, improve endurance, prepare for functional activities.
-
Activities:
- Progressive Resistance Exercises: Using therapy putty, resistance bands, light weights for wrist flexion/extension, radial/ulnar deviation, pronation/supination.
- Isotonic and Isometric Exercises: Tailored to individual needs.
- Endurance Training: Repetitive low-resistance tasks.
- Advanced Tendon Gliding: More dynamic tendon-specific exercises.
4. Return to Activity Phase (Advanced Phase)
- Initiation: Typically 3-6 months post-operatively, depending on the procedure and patient progress.
- Goals: Achieve maximal functional recovery, return to work, sports, and daily activities without restrictions.
-
Activities:
- Sport-Specific Training: Gradual reintroduction of activities, emphasizing proper technique and protective equipment.
- Work Simulation: Occupational therapy for work-specific tasks.
- Impact Loading: Gradual introduction of weight-bearing and impact activities, with caution.
- Proprioceptive Training: Balance and coordination exercises.
Specific Considerations:
- Dorsal Distal Radius Fractures: Immobilization often 4-6 weeks, followed by gradual mobilization. Emphasis on restoring pronation/supination and avoiding EPL rupture.
- Scaphoid Non-unions: Longer immobilization (typically 8-12 weeks or until radiographic union) due to delayed healing potential. Strengthening progresses slowly.
- Arthrodesis: Immobilization until radiographic fusion is confirmed (often 8-12+ weeks). Focus shifts from motion to strength and endurance in the fused wrist.
- Ganglion Excision: Short period of immobilization (e.g., 1 week), followed by early range of motion to prevent stiffness and recurrence.
Close collaboration between the surgeon, hand therapist, and patient is crucial to adapt the protocol to individual progress and ensure safe, effective rehabilitation.
Summary of Key Literature / Guidelines
The dorsal approach to the wrist remains a cornerstone in orthopedic and hand surgery, with a rich body of literature guiding its application and refinement.
- Extensor Compartments: Early anatomical studies by Quervain (1895) and subsequent detailed dissections established the understanding of the six extensor compartments. This foundational knowledge is essential for surgical planning, as detailed in standard anatomical texts (e.g., Netter, Gray's Anatomy) and surgical atlases (e.g., Operative Hand Surgery by Green's, Campbell's Operative Orthopaedics). The biomechanical role of the extensor retinaculum in preventing bowstringing is widely accepted, influencing decisions regarding its repair or release.
- Neurovascular Protection: The vulnerability of the superficial radial nerve during dorsal wrist surgery has been consistently highlighted in the literature. Studies by Stahl and Wolff (2000) and Dellon (1986) emphasize the variable course of the SRN and the need for meticulous dissection and careful retraction to minimize the risk of iatrogenic injury and subsequent neuroma formation. The routine identification and protection of this nerve are considered a critical step in the dorsal approach.
- Distal Radius Fractures: While volar plating has become the dominant fixation method for most distal radius fractures, the dorsal approach maintains its relevance for specific fracture patterns. Classic indications include highly comminuted dorsal articular fractures, dorsal shearing fractures, and revision of failed volar plating. Studies by Jupiter et al. (2006) and Medoff et al. (2015) describe dorsal plating techniques and considerations for achieving articular reduction and stable fixation, while acknowledging the higher rates of soft tissue irritation, particularly EPL rupture. Evolution in dorsal plate design (e.g., lower profile, pre-contoured) aims to mitigate these complications.
- Scaphoid Non-unions: The dorsal approach is favored for treating scaphoid non-unions, especially those involving the proximal pole or requiring vascularized bone grafting. Literature by Matti (1937), Russe (1960), and more recently by Mathoulin et al. (2015) and others, detail techniques for débridement, bone grafting (e.g., dorsal intercarpal artery pedicled bone graft), and internal fixation, often with headless compression screws. The choice of graft and approach depends on factors such as scaphoid viability, humpback deformity, and fragment size.
- Dorsal Wrist Arthrodesis: For advanced wrist arthritis, particularly "SLAC" (Scapholunate Advanced Collapse) and "SNAC" (Scaphoid Non-union Advanced Collapse) wrists, four-corner arthrodesis via a dorsal approach is a well-established salvage procedure. Seminal work by Watson and Ballet (1984) and more recent reviews confirm its efficacy in providing pain relief and maintaining reasonable wrist motion. Total wrist arthrodesis, also commonly performed dorsally, is reserved for end-stage pan-carpal arthritis or severe instability.
- Dorsal Ganglion Excision: Surgical excision of dorsal wrist ganglions, as described by Angelides and Wallace (1976), remains a common procedure. Studies consistently show lower recurrence rates with open excision compared to aspiration, though the recurrence rate for open excision can still be up to 5-10%.
- Retinacular Repair: The debate regarding the extent of retinacular repair (complete, partial, or none) continues. While complete repair aims to prevent bowstringing, particularly of the EDC, some surgeons advocate for partial repair or even excision of a portion of the retinaculum over certain compartments (e.g., fourth compartment for synovectomy) to minimize tendon irritation or nerve entrapment, especially after dorsal plating. Current practice often favors a loose repair or Z-plasty lengthening to achieve adequate coverage without excessive tension.
- Guidelines: Professional organizations such as the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH) provide clinical practice guidelines for the management of conditions frequently addressed via a dorsal approach (e.g., distal radius fractures, scaphoid fractures), implicitly endorsing or outlining surgical considerations that often involve this exposure.
Future research will likely continue to focus on optimizing plate designs to minimize hardware-related soft tissue complications, refining techniques for biological augmentation in non-union treatment, and improving rehabilitation protocols to accelerate functional recovery while safeguarding surgical repairs. The dorsal approach, with its direct exposure and versatility, will undoubtedly remain a critical tool in the orthopedic surgeon's armamentarium.
Clinical & Radiographic Imaging