Unlock Safe Access: The Anterolateral Approach to the Lateral Tibial Plateau
Introduction & Epidemiology
Tibial plateau fractures represent a significant challenge in orthopedic trauma, comprising approximately 1% of all fractures and 8% of fractures in the elderly. These complex intra-articular injuries are characterized by disruption of the articular surface, often with associated metaphyseal comminution, soft tissue compromise, and potential ligamentous or meniscal damage. The incidence exhibits a bimodal distribution, affecting young males involved in high-energy trauma (e.g., motor vehicle accidents, falls from height) and older females with osteoporotic bone following low-energy falls. The prognosis is directly correlated with the restoration of articular congruence, axial alignment, and overall knee stability. Failure to achieve these goals can lead to debilitating post-traumatic osteoarthritis, chronic pain, and functional impairment.
The optimal management of tibial plateau fractures necessitates a thorough understanding of the fracture morphology, the surrounding soft tissue envelope, and the intricate biomechanics of the knee joint. Surgical intervention, primarily open reduction and internal fixation (ORIF), is frequently required to achieve anatomical reduction and stable fixation, particularly for displaced articular fractures. Various surgical approaches have been described for addressing tibial plateau fractures, each with specific advantages and disadvantages depending on the fracture pattern and surgeon preference.
The anterolateral approach to the lateral tibial plateau is a workhorse approach, offering safe and reliable access to the lateral articular surface and metaphysis. Its utility extends beyond acute fracture fixation to include revision surgery for malunion or nonunion, treatment of localized osteomyelitis, excision or biopsy of tumors, and harvesting of local bone graft. This approach is preferred over a direct anterior incision due to its favorable soft tissue handling, reduced risk of wound complications, and excellent visualization of the critical lateral articular surface. Meticulous pre-operative planning, precise surgical technique, and a structured rehabilitation protocol are paramount to achieving successful outcomes.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the regional anatomy and biomechanics is fundamental for successful management of lateral tibial plateau fractures via the anterolateral approach.
Bony Anatomy
The proximal tibia consists of a broad superior articular surface, divided into medial and lateral tibial plateaus by the intercondylar eminence. The lateral tibial plateau is generally smaller and more convex than the medial plateau, allowing for greater external rotation of the tibia relative to the femur during knee flexion. The articular cartilage of the lateral plateau is thickest centrally and posteriorly. Inferior to the articular surface, the lateral condyle exhibits a strong cortical buttress, which resists varus forces and provides a robust platform for plate fixation. The fibular head articulates with the posterolateral aspect of the tibia via the proximal tibiofibular joint, a critical landmark for nerve identification.
Soft Tissue Anatomy
The soft tissue covering of the proximal tibia is notoriously thin and delicate, particularly anteriorly and anterolaterally. It comprises:
*
Skin and Subcutaneous Tissue:
Directly overlying the bone with minimal muscle bulk, making it highly susceptible to injury from trauma and surgical insult. Massive swelling, blistering, and even necrosis can occur, particularly after high-velocity trauma.
*
Deep Fascia:
The investing fascia of the lower leg, which proximally incorporates the fascia lata and distally encases the muscles of the anterior and lateral compartments.
*
Muscles:
*
Anterior Compartment:
Primarily the tibialis anterior, extensor digitorum longus (EDL), extensor hallucis longus (EHL), and peroneus tertius. These muscles are innervated by the deep peroneal nerve.
*
Lateral Compartment:
Peroneus longus and brevis, situated lateral to the anterior compartment, superficial to the fibula. These are innervated by the superficial peroneal nerve.
*
Iliotibial Band (ITB):
A thick, fibrous band that runs along the lateral thigh, inserting distally onto Gerdy's tubercle on the anterolateral aspect of the tibia. It provides significant lateral stability to the knee.
*
Ligamentous Structures:
*
Lateral Collateral Ligament (LCL):
Extends from the lateral femoral epicondyle to the fibular head, providing primary restraint to varus stress.
*
Popliteus Tendon:
Originates from the lateral femoral condyle, passes deep to the LCL, and inserts on the posterior aspect of the tibia.
*
Menisci:
The lateral meniscus is typically more mobile than the medial and is often involved in lateral tibial plateau fractures, either entrapped within the fracture or avulsed. The meniscotibial (coronary) ligaments anchor the meniscus to the tibial plateau.
Neurovascular Anatomy
- Common Peroneal Nerve: This nerve is of paramount importance during the anterolateral approach. It courses superficially, wrapping around the fibular neck, where it is highly vulnerable to direct trauma, compression, or iatrogenic injury during dissection or hardware placement. It then divides into the superficial and deep peroneal nerves, innervating the lateral and anterior leg compartments, respectively. Injury can result in foot drop and sensory deficits.
- Anterior Tibial Artery and Vein: Located deep within the anterior compartment, usually well protected by the muscle belly of the tibialis anterior. While typically not directly exposed, care must be taken with deep retractors or aggressive dissection, particularly in the distal aspect of the exposure.
Biomechanics of the Lateral Tibial Plateau
The lateral tibial plateau bears approximately 60% of the body weight during standing. Its articular surface, along with the lateral meniscus, is crucial for load transmission and maintaining knee stability through the gait cycle. Fractures of the lateral plateau often result from a combination of axial loading and valgus stress, leading to impaction and depression of the articular surface, often with associated lateral meniscal tears. The degree of articular incongruity, metaphyseal collapse, and associated ligamentous instability dictates the functional outcome. Restoration of the articular surface to within 1-2 mm of anatomical congruence and re-establishment of mechanical axis are critical to prevent progressive degenerative changes.
Indications & Contraindications
The anterolateral approach is a versatile approach primarily utilized for conditions affecting the lateral tibial plateau.
Indications for Operative Management via Anterolateral Approach
-
Open Reduction and Internal Fixation (ORIF) of Fractures of the Lateral Tibial Plateau:
This is the most common indication, particularly for Schatzker Type I, II, and III fractures, and AO/OTA 41-B1, B2, B3 fracture patterns. It allows for direct visualization of the articular surface, elevation of depressed fragments, and stable buttress plating.
- Displaced articular fractures (typically >2mm step-off or >5mm depression).
- Fractures with significant metaphyseal comminution requiring structural support.
- Fractures associated with significant knee instability.
- Bicondylar fractures with a major lateral component where the lateral side needs to be addressed first.
- Bone Grafting for Delayed Union and Nonunion of Fractures: In cases of persistent delayed union or established nonunion of lateral tibial plateau fractures, this approach facilitates debridement of the nonunion site and placement of autogenous or allogeneic bone graft.
- Treatment of Osteomyelitis: For localized osteomyelitis involving the lateral tibial plateau, the approach provides direct access for debridement of infected bone and soft tissue.
- Excision and Biopsy of Tumors: Benign or malignant tumors of the proximal lateral tibia can be accessed for biopsy or en bloc excision, with adequate margins.
- Harvesting of Bone Graft: While often harvested from the iliac crest, local cancellous bone graft can sometimes be harvested from the proximal tibia via this approach for minor defects.
- Concurrent Meniscal and Ligamentous Repair: The approach allows for direct visualization and repair of lateral meniscal tears or peripheral detachments and, in some cases, can facilitate repair of associated lateral collateral ligament injuries.
Contraindications
- Severe Soft Tissue Compromise: Massive swelling, extensive blistering, necrotic skin, or active infection overlying the proposed incision site are relative contraindications for immediate definitive ORIF. Delaying surgery to allow soft tissue recovery is often prudent.
- Open Fractures (Gustilo Type IIIB or IIIC): While often requiring initial debridement and external fixation, definitive internal fixation via this approach may be delayed or contraindicated if extensive soft tissue coverage is required.
- Fractures Amenable to Non-Operative Management: Minimally displaced, stable fractures without significant articular step-off, or fractures in patients with severe comorbidities precluding surgery may be managed non-operatively.
- Isolated Posteromedial or Pure Posterior Fractures: These patterns are better accessed via posteromedial, direct posterior, or combined approaches.
- Extremely Fragile Bone Quality: In severe osteoporosis, stable fixation may be challenging, and alternative strategies (e.g., external fixation, less invasive internal fixation) may be considered.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Displacement | Displaced articular fractures (>2mm step-off, >5mm depression) | Minimally displaced fractures (<2mm step-off, <5mm depression) |
| Fracture Stability | Unstable fractures (e.g., significant metaphyseal comminution, associated ligamentous instability) | Stable fractures, non-articular fractures (e.g., isolated fibular head) |
| Associated Injuries | Ligamentous instability requiring repair, meniscal incarceration | Stable knee with intact ligaments or amenable to bracing |
| Soft Tissue Status | Recovered, closed soft tissues without significant swelling or blistering | Severe swelling, active infection, open fractures (initial external fixation often followed by delayed ORIF) |
| Patient Factors | Physiologically fit, compliant for rehabilitation, high functional demands | Significant comorbidities, non-compliant, severe osteoporosis, low functional demands |
| Specific Pathology | Delayed union/nonunion, osteomyelitis, tumor excision | Asymptomatic nonunion, localized pain managed conservatively |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for successful surgical outcomes and minimizing complications.
Pre-Operative Planning
- Detailed History and Physical Examination: Assess mechanism of injury, comorbidities, neurovascular status, and soft tissue envelope. Document any pre-existing nerve deficits or vascular compromise.
-
Imaging Studies:
- Plain Radiographs: AP, lateral, oblique views of the knee (45° internal and external rotation obliques) are initial studies. Traction views can help delineate fracture lines and articular depression.
- Computed Tomography (CT) Scan: Essential for definitive surgical planning. Provides detailed information on fracture morphology, articular step-off and depression, comminution, fragment size and location, and associated fibular head fractures. 3D reconstructions are invaluable for visualizing complex fracture patterns.
- Magnetic Resonance Imaging (MRI): Indicated if significant ligamentous or meniscal injury is suspected, as these findings can influence surgical approach and repair strategy.
- Soft Tissue Assessment: Critical to assess the condition of the skin, subcutaneous tissue, and muscle. The presence of significant swelling, blistering, or an open wound may necessitate a delay in definitive ORIF, often managed initially with spanning external fixation. The Tscherne classification for closed soft tissue injuries or Gustilo-Anderson classification for open fractures guides management.
- Surgical Strategy Development: Based on imaging, determine the appropriate plate type (e.g., precontoured lateral locking plate, T-plate, L-plate), plate length, screw trajectories, and potential need for bone graft (autograft, allograft, synthetic). Pre-bending plates or planning screw placement using templates can be beneficial.
- Antibiotic Prophylaxis: Administer pre-operative intravenous antibiotics in accordance with institutional guidelines.
- Anesthesia: General anesthesia is typically employed, though regional anesthesia can be considered.
Patient Positioning
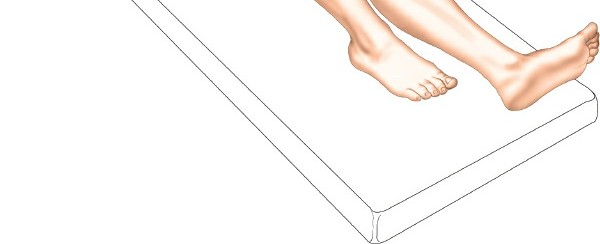
-
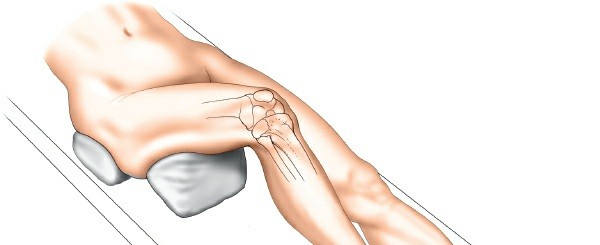
Supine Position:
The patient is placed supine on a radiolucent operating table.
This image likely depicts the initial supine patient positioning. - Knee Flexion: A firm, padded wedge or bump is placed beneath the knee to flex the joint to approximately 60 degrees. This maneuver relaxes the gastrocnemius muscle, facilitates easier knee flexion during the case, and allows for improved exposure of the posterior aspect of the lateral plateau.
- Buttock Bolster: A small bag or bolster is placed underneath the ipsilateral buttock. This helps to internally rotate the limb slightly, preventing external rotation and ensuring the knee is optimally positioned for an anterolateral incision.
- Tourniquet: A pneumatic tourniquet is applied high on the proximal thigh.
- Fluoroscopy Access: Ensure unrestricted access for intraoperative fluoroscopy in AP, lateral, and oblique planes to confirm reduction and hardware placement.
- Draping: The leg should be draped free to allow full range of motion of the knee and hip throughout the procedure, enabling dynamic assessment and manipulation. The operative field should be prepped widely from the mid-thigh to the foot.
Detailed Surgical Approach / Technique
The anterolateral approach offers excellent exposure of the lateral tibial plateau, permitting direct visualization of the articular surface and stable fixation.
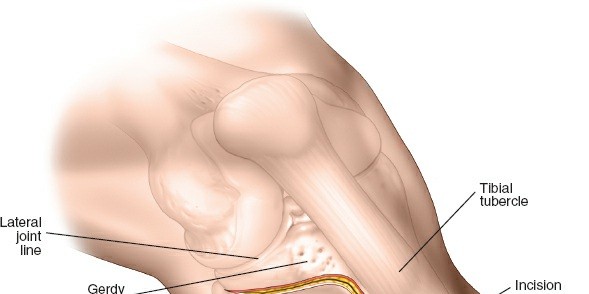
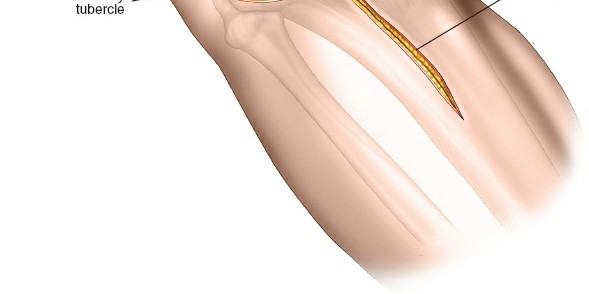
1. Incision
The incision is typically a curvilinear or longitudinal incision, approximately 10-15 cm in length, depending on the extent of fracture and desired exposure.
*
Proximal Starting Point:
Begins just anterior to the lateral femoral epicondyle or lateral joint line.
*
Course:
Curves gently anteriorly over the joint line, then extends distally along the anterolateral aspect of the tibia, approximately 1 cm lateral to the anterior crest.
*
Important Consideration:
The incision should not directly overly the planned plate position if possible, to provide a healthy soft tissue envelope over the hardware.

This image likely shows the skin incision outline or initial skin incision.
2. Superficial Dissection
- Skin and Subcutaneous Tissue: The incision is carried through the skin and subcutaneous tissue. Meticulous hemostasis is achieved.
- Deep Fascia: The deep fascia of the leg (fascia lata proximally, investing fascia of the tibialis anterior distally) is identified and incised longitudinally. Care is taken to identify and protect any superficial cutaneous nerves, though significant branches are less common in this specific interval.
- Skin Flaps: Subfascial elevation of full-thickness skin and subcutaneous tissue flaps is performed to expose the underlying musculature. The anterior flap is retracted anteriorly, and the posterior flap laterally, taking care to maintain flap thickness to preserve vascularity.
3. Exposure of the Lateral Compartment
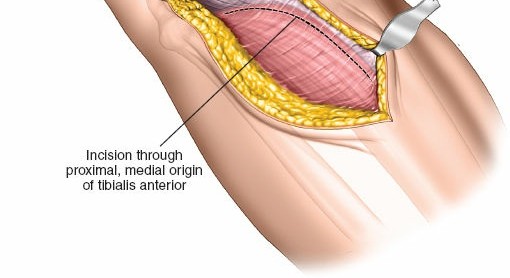
- Identify Muscles: The anterior border of the tibialis anterior muscle (anterior compartment) is identified. Lateral to this, the muscles of the lateral compartment (extensor digitorum longus, peroneus longus, and brevis) are visible.
- Internervous Plane: The surgical plane is developed between the tibialis anterior (supplied by the deep peroneal nerve) and the extensor digitorum longus (also supplied by the deep peroneal nerve). This is not a true internervous plane but rather an intermuscular interval within the anterior compartment, or sometimes the interval between the anterior compartment and the lateral compartment (peroneus longus and brevis, supplied by the superficial peroneal nerve). The key is to reflect the tibialis anterior medially.
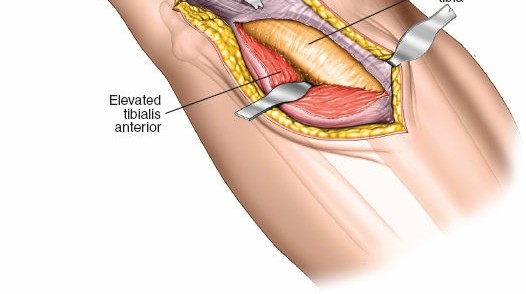
- Subperiosteal Elevation: The periosteum over the lateral tibial metaphysis is incised, and the muscles of the anterior compartment (tibialis anterior) are elevated subperiosteally from the anterolateral surface of the tibia, reflecting them anteriorly and medially.
- Gerdy's Tubercle: Proximally, the iliotibial band (ITB) attaches to Gerdy's tubercle. The ITB can be either longitudinally incised or elevated off Gerdy's tubercle and retracted anteriorly or posteriorly. For most lateral plateau fractures, anterior reflection of the ITB, often by incising its anterior attachment at Gerdy's tubercle, is preferred to gain optimal access to the articular surface.
4. Deep Dissection & Common Peroneal Nerve Protection
- Fibular Head Identification: The fibular head and neck are important landmarks, located posteriorly and laterally relative to the proximal tibia.
-
Common Peroneal Nerve:
Critical Step:
The common peroneal nerve courses around the fibular neck. It must be identified visually or by palpation and carefully protected. The nerve typically lies just posterior to the posterolateral aspect of the fibular neck. Retraction should be gentle and directly on muscle or bone, avoiding direct pressure on the nerve.
This image likely depicts the deeper dissection, highlighting the fibular head and potentially the common peroneal nerve. - Subperiosteal Elevation (Lateral Aspect): The muscles of the lateral compartment (extensor digitorum longus and peroneus longus) are further elevated subperiosteally and retracted laterally and posteriorly from the lateral tibial metaphysis. This exposes the lateral capsule and the lateral aspect of the tibial plateau.
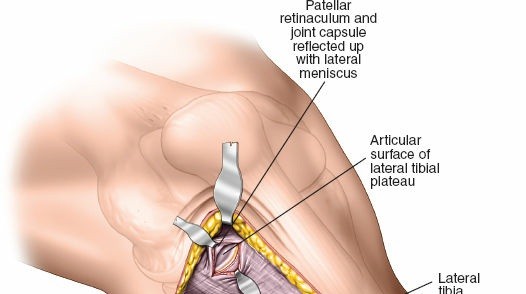
5. Arthrotomy & Meniscal Management
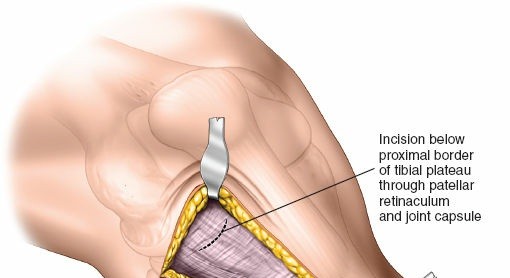
- Capsular Incision: The anterolateral knee joint capsule is incised longitudinally to expose the fracture site and the lateral meniscus.
- Meniscal Assessment: The lateral meniscus is carefully inspected. In lateral tibial plateau fractures, the meniscus is often detached peripherally (meniscotibial ligament avulsion) or entrapped within the fracture fragments.
-
Meniscal Management:
To achieve direct visualization and reduction of the articular surface, the lateral meniscus often needs to be mobilized. This is typically achieved by incising the meniscotibial ligament peripherally. The meniscus is then retracted superiorly with stay sutures or a small hook, providing a clear view of the depressed articular fragments. Preservation of meniscal attachments is paramount if possible, and any detachments should be repaired at the end of the case.
This image likely shows the arthrotomy and meniscal elevation for fracture visualization.
6. Fracture Reduction
- Temporary Fixation/Distraction: Temporary K-wires can be used to stabilize large peripheral fragments. A femoral distractor or external fixator across the knee joint can be applied to distract the joint, aiding visualization and reduction of impacted fragments, and restoring overall limb length.
- Cortical Window (Optional): For deeply depressed fragments, a small cortical window may be created in the lateral metaphyseal bone, just inferior to the articular surface, to facilitate elevation. Alternatively, the existing fracture lines can be utilized.
- Fragment Elevation: Specialized elevators (e.g., broad osteotomes, lamina spreaders, bone tampers) are carefully inserted through the cortical window or fracture site. The depressed articular fragments are then gently elevated under direct vision (via the arthrotomy) to restore the anatomical contour of the articular surface.
-
Subchondral Support & Bone Grafting:
Once elevated, the metaphyseal void created beneath the reduced articular fragments is packed with bone graft to provide structural support and prevent re-collapse. Autogenous cancellous bone graft (harvested from the iliac crest, greater trochanter, or locally from the proximal tibia) is the gold standard. Allograft (e.g., cancellous chips) or synthetic bone graft substitutes can also be used.
This image likely illustrates the elevation of depressed fragments and subsequent bone grafting. - Confirmation of Reduction: Articular reduction is confirmed visually and by fluoroscopy (AP and lateral views).
7. Internal Fixation
-
Plate Application:
A precontoured lateral tibial plateau plate (e.g., locking plate, buttress plate) is selected and applied to the lateral aspect of the tibia. The plate should be positioned to act as a buttress against varus collapse and to support the elevated articular segment. Plate position and length are confirmed with fluoroscopy.
This image likely demonstrates the application of a precontoured lateral tibial plateau plate. -
Screw Placement:
- Subchondral Screws: Cancellous screws are typically directed from the plate through the metaphyseal bone to engage and support the elevated articular fragments, providing subchondral support. These screws are placed under fluoroscopic guidance to ensure they do not penetrate the articular surface.
- Lag Screws: For large, reducible fragments, lag screws can be used to achieve interfragmentary compression.
- Locking Screws: In osteoporotic bone or comminuted fractures, locking screws are employed to create an angularly stable construct, providing enhanced fixation stability.
-
Distal Fixation:
Cortical screws or locking screws are placed distally into the tibial diaphysis to secure the plate.
This image likely shows screw placement, emphasizing the use of fluoroscopy to verify trajectory and length.
- Final Stability Assessment: After definitive fixation, the knee is put through a full range of motion, and varus/valgus stress is applied to assess stability. Fluoroscopy is used to confirm final reduction and hardware position.
8. Closure
- Irrigation: The wound is thoroughly irrigated with sterile saline.
- Meniscal Repair: If the lateral meniscus was detached, it should be repaired back to its peripheral attachments (meniscotibial ligament) using sutures.
- Deep Fascia: The deep fascia is closed with absorbable sutures.
- Subcutaneous Tissue: The subcutaneous layer is closed to obliterate dead space.
- Skin: The skin is closed with staples or non-absorbable sutures.
- Drainage: A surgical drain may be placed in cases of significant bleeding or dead space.
-
Dressing and Immobilization:
A sterile dressing is applied, and the knee is immobilized in a hinged knee brace or splint, typically in full extension or slight flexion.
This image likely represents the final fixation and wound closure.
Complications & Management
Despite meticulous surgical technique, complications can arise following the anterolateral approach to the lateral tibial plateau. Early recognition and appropriate management are crucial for optimizing patient outcomes.
General Complications
- Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE): Risk is increased in trauma patients. Prophylaxis with chemical agents (e.g., low molecular weight heparin) and mechanical devices (e.g., intermittent pneumatic compression) is standard.
- Neurovascular Injury: Although rare, injury to the anterior tibial artery or vein can occur.
- Compartment Syndrome: While not specific to the anterolateral approach, proximal tibia fractures are at high risk. Vigilance for the "6 Ps" (Pain, Pallor, Pulselessness, Paresthesia, Paralysis, Poikilothermia) and emergent fasciotomy are critical.
Specific Complications Related to Tibial Plateau Fractures and the Anterolateral Approach
| Complication | Incidence (%) | Salvage Strategy |
|---|---|---|
| Infection | 2-10 | Aggressive surgical debridement, culture-specific intravenous antibiotics, hardware retention (if stable and early) or removal (if unstable/chronic), soft tissue coverage (flaps) |
| Wound Complications | 5-15 | Local wound care, serial debridement, negative pressure wound therapy, skin grafting, flap reconstruction (pedicled or free) |
| Loss of Reduction/Malunion | 5-20 | Early revision ORIF, corrective osteotomy, bracing; for mild malunion, often conservative management. |
| Post-Traumatic Arthritis | 20-50 | Conservative management (NSAIDs, activity modification, bracing), arthroscopy for debridement, osteotomy (high tibial osteotomy for varus malalignment), unicompartmental or total knee arthroplasty |
| Stiffness/Loss of ROM | 10-30 | Intensive physical therapy, manipulation under anesthesia (MUA), arthroscopic or open arthrolysis |
| Common Peroneal Nerve Palsy | 0.5-5 | Observation (if neuropraxia), nerve exploration and neurolysis/repair (if severe injury/transection), tendon transfer for functional deficits, ankle-foot orthosis (AFO) |
| Nonunion/Delayed Union | 2-10 | Revision fixation, autogenous bone grafting (iliac crest), allograft, bone morphogenetic proteins (BMPs), electrical stimulation |
| Hardware Prominence | 5-15 | Elective hardware removal after fracture union |
| Vascular Injury (Popliteal Artery) | <1 | Emergent vascular repair, fasciotomy if ischemia/reperfusion injury |
Management Considerations
- Soft Tissue Necrosis: This is a particularly vexing complication due to the thin soft tissue envelope. Prevention involves careful handling, minimal retraction, adequate skin bridges, and delayed surgery when initial swelling or blistering is severe. Management often requires plastic surgical consultation for local or free flap coverage.
- Post-Traumatic Arthritis: This is the most common long-term sequela. Factors contributing include residual articular incongruity (>1-2 mm), axial malalignment, meniscal injury, and associated chondral damage. While surgical correction aims to mitigate this, some degree of arthritis is often inevitable.
- Common Peroneal Nerve Injury: Due to its superficial course around the fibular neck, the common peroneal nerve is susceptible. Careful identification and gentle retraction are paramount. If a new foot drop occurs post-operatively, conservative management with an AFO is often initiated if electrodiagnostic studies suggest neuropraxia. Surgical exploration may be warranted for persistent deficits or suspected direct injury.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as crucial as the surgical technique itself for achieving optimal functional recovery and preventing long-term complications. Protocols are individualized based on fracture type, fixation stability, associated injuries (e.g., meniscal repair, ligamentous injury), and patient factors (e.g., bone quality, compliance).
Phase I: Early Protection and Motion (Weeks 0-6)
- Goals: Control pain and swelling, protect fracture fixation, initiate early passive range of motion (PROM).
- Weight-Bearing: Strictly non-weight bearing (NWB) to toe-touch weight-bearing (TTWB) on the operative leg. Crutches or a walker are used for ambulation.
-
Immobilization:
- Hinged knee brace worn at all times (except during exercises and hygiene).
- Initially locked in full extension or slight flexion (e.g., 0-30 degrees) for the first 2-4 weeks to protect fixation and soft tissue.
- Gradually increase flexion as per surgeon's discretion, typically allowing 0-90 degrees by 6 weeks.
-
Exercises:
- Cryotherapy and Elevation: Frequent application of ice and elevation to reduce swelling.
- Ankle Pumps: Promote circulation and prevent DVT.
- Quadriceps Sets/Isometrics: Maintain muscle tone without knee movement.
- Gentle Passive ROM: Manual therapy by a physical therapist or continuous passive motion (CPM) machine, starting with a limited arc (e.g., 0-30 degrees) and gradually increasing.
- Upper Extremity Strengthening: For crutch use.
- Specific Considerations: If meniscal repair was performed, ROM and weight-bearing progression may be more restricted.
Phase II: Progressive Weight-Bearing and Strengthening (Weeks 6-12)
- Goals: Progress weight-bearing, increase range of motion, initiate active strengthening.
- Weight-Bearing: Gradual progression from TTWB to partial weight-bearing (PWB) (e.g., 25-50% body weight) as per radiographic evidence of fracture healing and clinical stability. Full weight-bearing (FWB) is typically achieved by 12 weeks, but can be delayed based on fracture complexity and bone healing.
- Immobilization: Continue hinged knee brace for support during ambulation, often unlocked for full ROM.
-
Exercises:
- Active Range of Motion (AROM): Progress towards full knee flexion and extension.
-
Strengthening:
- Isometric exercises (e.g., wall sits, bridge holds).
- Isotonic exercises with light resistance (e.g., knee extensions, hamstring curls, straight leg raises).
- Closed-chain exercises (e.g., mini-squats, leg presses) as weight-bearing tolerance improves.
- Proprioception and Balance: Single-leg stance, balance board exercises.
- Gait Training: Focus on proper gait mechanics.
Phase III: Advanced Strengthening and Return to Activity (Weeks 12 - 6 Months+)
- Goals: Achieve full functional range of motion, maximal strength, and safe return to pre-injury activities.
- Weight-Bearing: Full weight-bearing without assistive devices.
- Brace: Discontinue brace use once strength and stability are sufficient.
-
Exercises:
- Advanced Strengthening: Progress resistance and intensity of exercises. Include plyometrics and sport-specific drills if appropriate.
- Endurance Training: Cycling, swimming, elliptical.
- Agility Drills: Ladder drills, cone drills (for athletes).
- Return to Sport/High-Impact Activities: Typically not before 6 months post-surgery, and only after achieving full strength, stability, and clearance from the surgeon and physical therapist. Radiographic evidence of complete union is essential.
Key Rehabilitation Principles
- Individualization: Protocols must be tailored to the specific patient and injury.
- Pain-Guided Progression: Progression should be comfortable and pain-free.
- Protection of Fixation: Avoid aggressive movements or weight-bearing that could compromise the surgical construct.
- Early Motion: Essential to prevent stiffness and promote cartilage health, balanced with protection.
- Collaboration: Close communication between the surgeon, physical therapist, and patient is vital for successful outcomes.
Summary of Key Literature / Guidelines
The management of lateral tibial plateau fractures, particularly through the anterolateral approach, is guided by principles derived from extensive clinical experience and research. The primary objectives are anatomical reduction of the articular surface, stable internal fixation, and early, controlled mobilization.
Evolution of Treatment:
Historically, many tibial plateau fractures were treated non-operatively with prolonged traction or casting, often leading to poor outcomes characterized by malunion, stiffness, and post-traumatic arthritis. The advent of modern surgical techniques, improved implants, and a deeper understanding of fracture biomechanics, largely driven by the Arbeitsgemeinschaft für Osteosynthesefragen (AO) Foundation, revolutionized their management. The AO principles –
anatomical reduction, stable internal fixation, preservation of blood supply, and early functional mobilization
– are cornerstone tenets.
Role of Imaging:
Current guidelines universally emphasize the critical role of advanced imaging in surgical planning. While plain radiographs provide initial assessment,
computed tomography (CT) scans with 3D reconstructions
are indispensable for precisely delineating fracture morphology, quantifying articular depression and step-off, and identifying comminution, which directly informs surgical approach and fixation strategy. MRI is valuable for assessing concomitant meniscal and ligamentous injuries.
Anterolateral Approach Advantages:
Literature supports the anterolateral approach for its ability to provide direct visualization of the lateral articular surface, facilitating accurate reduction of depressed fragments. Studies have demonstrated its favorable soft tissue profile compared to more extensive anterior approaches, with generally lower rates of wound complications. A direct anterior approach often requires greater skin retraction over a fragile soft tissue envelope, increasing the risk of wound dehiscence and infection. The anterolateral incision, by being slightly off the primary bone, provides a healthier tissue bridge over the implant, thereby improving vascularity.
Fixation Principles:
*
Buttress Plating:
Lateral locking plates are commonly used to provide buttress support against axial loads and valgus stresses, resisting metaphyseal collapse. These plates, often precontoured, help restore the lateral cortical buttress.
*
Subchondral Support:
Cannulated or cancellous screws are strategically placed from the plate to support the elevated articular fragments, preventing re-collapse.
*
Bone Grafting:
Autogenous bone graft (most commonly from the iliac crest) remains the gold standard for filling metaphyseal voids created after elevating depressed articular fragments. Allograft or synthetic substitutes are viable alternatives.
Arthroscopy-Assisted Techniques:
Arthroscopy can be a valuable adjunct, particularly for confirming articular reduction, addressing meniscal tears, and assessing ligamentous integrity without further compromising the soft tissue envelope. However, it requires proficiency in combined open and arthroscopic techniques.
Management of Complex Fractures:
Bicondylar tibial plateau fractures (Schatzker Type V/VI, AO/OTA 41-C) often require combined or staged approaches. The anterolateral approach is frequently used to address the lateral side, sometimes in conjunction with a posteromedial or direct posterior approach for the medial or posteromedial fragments. Careful pre-operative planning is essential to ensure adequate skin bridges between incisions.
Outcomes and Complications:
Studies consistently report satisfactory to excellent functional outcomes in 70-80% of patients with lateral tibial plateau fractures treated with ORIF. However, post-traumatic arthritis remains the most common long-term complication, correlating significantly with residual articular incongruity, malalignment, and meniscal damage. Soft tissue complications, including wound breakdown and infection, are recognized challenges, particularly in high-energy injuries or those with significant initial soft tissue compromise. Meticulous surgical technique, staged procedures when necessary, and close attention to soft tissue viability are critical in minimizing these risks.
In conclusion, the anterolateral approach provides a reliable and effective means to address a spectrum of lateral tibial plateau pathologies. Adherence to established surgical principles, meticulous technique, and a structured post-operative rehabilitation program are paramount for achieving optimal patient outcomes and mitigating potential complications. The continuous evolution of implant technology and surgical strategies further refines the management of these challenging injuries.
Clinical & Radiographic Imaging