Mastering the Anterolateral Approach to Ankle and Hindpart
Introduction & Epidemiology
The anterolateral approach to the ankle and hindfoot is a versatile and commonly utilized surgical corridor, providing excellent access to the distal fibula, lateral distal tibia, talus, subtalar joint, and portions of the calcaneus and cuboid. Its strategic placement between distinct muscle compartments minimizes neurovascular risk when executed precisely. This approach is indispensable for a wide array of orthopedic pathologies, ranging from acute traumatic injuries such as ankle and hindfoot fractures, dislocations, and syndesmotic disruptions, to chronic conditions including ankle instability, osteochondral lesions of the talus (OCLTs), anterior ankle impingement, arthrodesis, and tumor resections.
Epidemiologically, ankle fractures represent a significant burden, with an incidence of 100-200 per 100,000 person-years, varying with age and activity level. Approximately 70% of these involve the lateral malleolus, frequently requiring direct visualization and internal fixation. Talar fractures, while less common (occurring in 0.3-0.6% of all fractures), often present with high-energy mechanisms and frequently necessitate open reduction and internal fixation to restore articular congruity and prevent long-term sequelae such as avascular necrosis or post-traumatic arthritis. Subtalar joint pathologies, including calcaneal anterior process fractures or subtalar instability, also benefit from this access. The proficiency in executing the anterolateral approach is therefore fundamental for any orthopedic surgeon managing foot and ankle trauma and degenerative conditions.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is paramount for safe and effective utilization of the anterolateral approach.
Osteology
The primary bony structures encountered or accessed via this approach include:
*
Distal Fibula
: Forms the lateral malleolus, a key landmark and often the focus of fixation.
*
Distal Tibia
: Specifically the anterolateral aspect and plafond, relevant for pilon fractures, syndesmotic injuries, and ankle arthrodesis.
*
Talus
: The talar body, neck, and head are extensively visualized. This approach is crucial for managing talar fractures and osteochondral lesions.
*
Calcaneus
: The anterior process and a portion of the lateral body are accessible, particularly useful for subtalar joint exposure.
*
Cuboid & Navicular
: The lateral aspect of the cuboid and its articulation with the calcaneus and fourth/fifth metatarsals, as well as the talonavicular joint, can be reached.
*
Metatarsals
: The base of the fifth metatarsal is a distal landmark, often considered the distal extent of the approach.
Ligamentous Structures
Key ligaments in the field:
*
Ankle Syndesmosis
: The anterior inferior tibiofibular ligament (AITFL) is often directly visualized and can be repaired or reduced.
*
Lateral Collateral Ligament Complex
: The anterior talofibular ligament (ATFL) is directly in the surgical field. The calcaneofibular ligament (CFL) and posterior talofibular ligament (PTFL) are posterior to the approach but their insertions can be accessed.
*
Capsule
: The anterior and lateral ankle joint capsule.
*
Subtalar Joint Capsule
: Provides access to the subtalar joint.
*
Bifurcate Ligament
: Connecting the calcaneus to the cuboid and navicular.
Musculotendinous Structures
The approach exploits an internervous plane between two major muscle compartments:
*
Anterior Compartment
: Contains the tibialis anterior, extensor hallucis longus (EHL), extensor digitorum longus (EDL), and peroneus tertius (PT). These muscles are supplied by the
deep peroneal nerve
. The EDL and PT are typically retracted medially/anteriorly. The extensor digitorum brevis (EDB), originating from the calcaneus, crosses the field more distally and often requires partial detachment or reflection.
*
Lateral Compartment
: Contains the peroneus longus (PL) and peroneus brevis (PB) tendons. These are supplied by the
superficial peroneal nerve
. These tendons are typically retracted posteriorly.
Neurovascular Structures
Understanding the precise location of nerves and vessels is critical to minimize iatrogenic injury.
*
Nerves
:
*
Superficial Peroneal Nerve (SPN)
: This nerve is the most vulnerable structure in the anterolateral approach. It emerges from the deep fascia in the distal third of the leg, typically 10-15 cm proximal to the tip of the lateral malleolus, dividing into the intermediate dorsal cutaneous nerve (IDCN) and medial dorsal cutaneous nerve. Its branches provide sensation to the dorsum of the foot, except for the first webspace (deep peroneal nerve) and lateral border (sural nerve). Careful identification and protection are paramount.
*
Deep Peroneal Nerve (DPN)
: Located deeper, within the anterior compartment, running with the anterior tibial artery. It supplies the anterior compartment muscles and sensation to the first webspace. It is generally protected by the anterior compartment muscles.
*
Sural Nerve
: Runs along the posterior aspect of the fibula and curves anteriorly to supply sensation to the lateral foot. It is usually posterior to the primary incision but can be at risk with extensive posterior dissection or retraction.
*
Arteries
:
*
Anterior Tibial Artery (ATA)
: Runs deep within the anterior compartment alongside the DPN.
*
Lateral Tarsal Artery
: A branch of the dorsalis pedis artery (distal continuation of ATA), often crosses the field near the origin of the EDB muscle and may require ligation or cauterization.
*
Perforating Branch of Peroneal Artery
: Located proximally, posterior to the fibula, connecting to the anterior circulation.
Internervous Plane
The key to the anterolateral approach lies in exploiting the internervous plane. As noted in the original seed content, this plane lies between the peroneal muscles (supplied by the superficial peroneal nerve) and the extensor muscles (supplied by the deep peroneal nerve; see
and

). By dissecting through the deep fascia along the anterior border of the fibula, the surgeon can retract the anterior compartment musculature anteromedially and the peroneal tendons posterolaterally, thus protecting both the deep and superficial peroneal nerves and their respective neurovascular bundles.
Biomechanics
Biomechanically, this approach allows direct visualization and manipulation of the ankle mortise, subtalar joint, and lateral column structures. It facilitates anatomical reduction of articular fractures, restoration of ligamentous integrity, and stable internal fixation under direct vision. The direct access to the lateral malleolus and syndesmosis is particularly advantageous for ankle fracture management.
Indications & Contraindications
Indications for the Anterolateral Approach
The anterolateral approach is indicated for a broad spectrum of pathologies requiring surgical intervention.
-
Traumatic Injuries
:
- Ankle Fractures : Lateral malleolus fractures (isolated or components of bimalleolar/trimalleolar patterns), anterior inferior tibial plafond fractures, pilon fractures with significant anterolateral involvement.
- Talar Fractures : Talar neck fractures (especially Hawkins type II/III/IV), talar body fractures, osteochondral lesions of the talus (OCLTs) requiring debridement, microfracture, or osteochondral autograft/allograft transplantation.
- Subtalar Fractures/Dislocations : Calcaneal anterior process fractures, subtalar joint dislocations requiring open reduction.
- Syndesmotic Injuries : Direct repair or stabilization of the anterior inferior tibiofibular ligament (AITFL) and syndesmotic reduction/fixation.
- Lisfranc Injuries : Midfoot instability, particularly with lateral column involvement.
-
Degenerative and Inflammatory Conditions
:
- Ankle Arthrodesis : Primary or revision procedures, particularly for lateral or global ankle arthritis.
- Ankle Arthroscopy (Access) : Can be used as a primary incision for anterior ankle debridement or osteophyte resection.
- Lateral Ankle Instability : Ligament repair (e.g., Broström-Gould procedure) or reconstruction.
- Anterior Ankle Impingement : Debridement of anterior osteophytes.
- Peroneal Tendon Pathology : Tenosynovectomy, debridement, or repair, especially if associated with lateral ankle instability.
-
Other
:
- Excision of soft tissue masses or osteophytes.
- Open biopsy of bony lesions.
Contraindications
While versatile, the anterolateral approach has relative and absolute contraindications:
-
Absolute Contraindications
:
- Active Infection : Cellulitis or osteomyelitis in the surgical field.
- Severe Soft Tissue Compromise : Extensive open wounds, severe blistering, or skin necrosis, which would preclude safe wound closure and increase infection risk.
-
Relative Contraindications
:
- Significant Pre-existing Peripheral Neuropathy : Especially if the superficial peroneal nerve is already compromised.
- Extensive Scarring : From previous surgeries or trauma, potentially obscuring anatomical planes and increasing the risk of neurovascular injury.
- Vascular Insufficiency : Severe peripheral artery disease that could compromise wound healing.
- Pathology Primarily Posterior or Medial : For example, isolated posterior malleolus fractures or purely medial ankle instability might be better served by a different approach or combined approaches.
Operative vs. Non-Operative Indications
The decision between operative and non-operative management is multifactorial and dependent on the specific pathology, patient factors, and surgeon experience.
| Pathology | Operative Indications | Non-Operative Indications |
|---|---|---|
| Lateral Malleolus Fractures | - Displaced, unstable fractures (≥2mm displacement) | - Nondisplaced or minimally displaced (≤2mm) stable fractures |
| - Bimalleolar or trimalleolar fractures | - Isolated fibular avulsion fractures without syndesmotic injury | |
| - Fractures with syndesmotic disruption | ||
| Pilon Fractures | - Displaced intra-articular fractures requiring anatomical reduction (anterolateral component) | - Nondisplaced or minimally displaced stable fractures (rare for pilon) |
| - Open fractures (after initial debridement) | - Severe soft tissue injury precluding immediate fixation (staged protocol) | |
| Talar Fractures (Neck/Body) | - Displaced talar neck fractures (Hawkins II, III, IV) due to high risk of AVN/malunion | - Nondisplaced talar neck or body fractures (rare, often still require close monitoring for AVN) |
| - Displaced talar body fractures (e.g., coronal, sagittal splits) | ||
| Osteochondral Lesions of Talus | - Symptomatic lesions unresponsive to conservative care | - Asymptomatic lesions, small lesions (<1 cm²) without significant subchondral edema, or those responding to activity modification, NSAIDs, and bracing. |
| - Larger lesions (>1.5 cm²), cystic lesions, or fragments requiring removal/fixation | ||
| Lateral Ankle Instability | - Chronic symptomatic instability unresponsive to 3-6 months of comprehensive non-operative treatment (bracing, physical therapy) | - Acute ankle sprains (initial management) |
| - Patients with recurrent ankle sprains significantly impacting quality of life or athletic performance | - Mild to moderate chronic instability responding to bracing and exercises. | |
| Ankle Arthrodesis | - Symptomatic end-stage ankle arthritis unresponsive to conservative management | - Mild ankle arthritis, pain managed with activity modification, NSAIDs, injections, bracing, or physical therapy. |
| Subtalar Dislocation/Fracture | - Irreducible closed dislocations (rare), open dislocations | - Closed, reducible dislocations (often require emergency reduction under sedation, but open approach may be needed if reduction fails) |
| - Displaced calcaneal anterior process fractures leading to impingement or instability | - Nondisplaced calcaneal anterior process fractures |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for optimizing surgical outcomes and minimizing complications.
Pre-operative Imaging
- Standard Radiographs : Anteroposterior (AP), lateral, and mortise views of the ankle, and AP/lateral/oblique views of the foot are standard. These provide initial assessment of fracture patterns, joint congruity, and presence of degenerative changes.
- Computed Tomography (CT) Scans : Crucial for complex fractures (pilon, talar, calcaneal), providing detailed information on fracture comminution, articular involvement, fragment rotation, and overall bone loss. 3D reconstructions are invaluable for pre-operative templating and understanding complex fracture morphology.
- Magnetic Resonance Imaging (MRI) : Indicated for suspected soft tissue injuries (ligamentous tears, osteochondral lesions, tendon pathology) or occult fractures not visible on plain radiographs or CT.
- Arteriography : Rarely needed, but considered in cases of severe trauma with suspected vascular injury or pre-existing peripheral vascular disease.
Surgical Environment & Equipment
- Operating Room Setup : Position image intensifier (fluoroscopy C-arm) on the contralateral side for optimal intraoperative views. Ensure availability of fracture tables or positioning devices if required for traction.
- Instrument Trays : Standard small fragment orthopedic set, dedicated foot and ankle sets (including specific reduction clamps, retractors, elevators), arthrodesis instrumentation if applicable, and tourniquet.
- Suture and Surgical Materials : Appropriate absorbable and non-absorbable sutures for deep and superficial closures, skin staples or sutures for skin, wound dressings, and post-operative immobilization (splints/casts).
Patient Positioning
- Supine Position : The patient is placed supine on the operating table.
- Affected Limb Positioning : The entire lower extremity should be prepped and draped to allow free manipulation of the foot and ankle, which is crucial for fracture reduction and intraoperative fluoroscopy.
-
Internal Rotation
:
As per seed content
, a large sandbag or bump is placed underneath the affected buttock or hip to facilitate internal rotation of the entire leg. This maneuver brings the lateral malleolus and the anterolateral aspect of the ankle forward, perpendicular to the floor, optimizing surgical access.
demonstrates this positioning. -
Exsanguination and Tourniquet
: The limb is exsanguinated either by elevation for 3 to 5 minutes or by applying a soft rubber bandage (Esmarch bandage). A pneumatic tourniquet is then inflated on the proximal thigh to achieve a bloodless field, typically to 250-300 mmHg.
shows the tourniquet in place. - Sterile Prep and Drape : Standard sterile preparation of the limb from the mid-thigh to the toes, ensuring a wide surgical field. Sterile adhesive drapes are applied, often utilizing a stockinette or impervious drape to isolate the foot and ankle.
Anesthesia and Antibiotic Prophylaxis
- Anesthesia : General anesthesia is commonly used, often supplemented with a regional anesthetic block (e.g., popliteal or ankle block) for post-operative pain management.
- Antibiotic Prophylaxis : Administer intravenous prophylactic antibiotics (e.g., Cefazolin) within 60 minutes prior to incision, according to institutional protocols, and continued as appropriate.
Detailed Surgical Approach / Technique
The anterolateral approach demands a methodical, layer-by-layer dissection to safely navigate through the anatomical structures and achieve optimal exposure.
1. Incision and Initial Landmarks
-
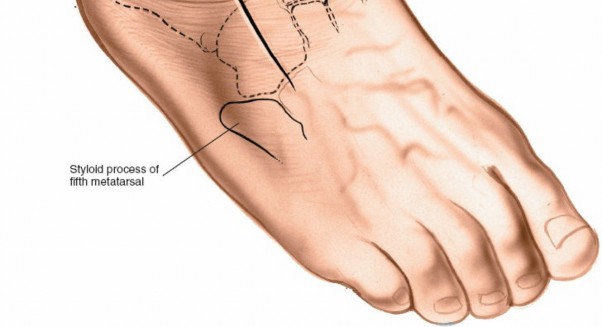
Landmarks
: Palpate the
lateral malleolus
at the distal subcutaneous end of the fibula. Distally, palpate the
base of the fifth metatarsal
, a prominent bony mass on the lateral aspect of the foot.
shows these landmarks. -
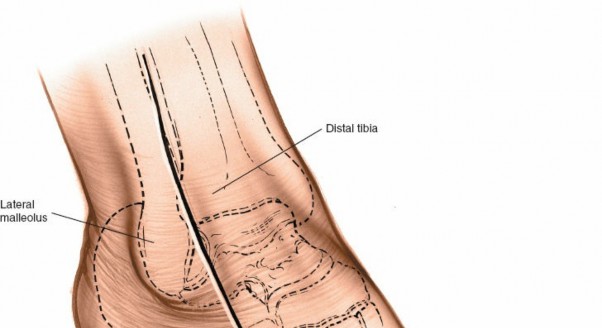
Incision Planning
: The incision is typically a longitudinal curvilinear incision, approximately 8-12 cm in length, centered over the anterior border of the distal fibula. It begins approximately 3-5 cm proximal to the tip of the lateral malleolus, curving distally and slightly anteriorly towards the sinus tarsi, and may extend further towards the base of the fifth metatarsal or cuboid, depending on the pathology and desired exposure.
illustrates an incision line. For conditions like talar neck fractures, it might be more anterior, whereas for lateral malleolus fractures, it can be directly over the anterior border of the fibula.
2. Superficial Surgical Dissection
- Skin and Subcutaneous Tissue : Incise the skin with a scalpel. Proceed cautiously through the subcutaneous tissue.
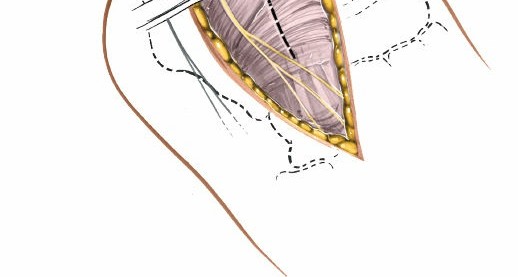
-
Identification of Superficial Peroneal Nerve (SPN)
: This is a critical step. The branches of the superficial peroneal nerve (intermediate dorsal cutaneous nerve, lateral dorsal cutaneous nerve) typically emerge through the deep fascia in the distal third of the leg, anterior to the fibula.
Carefully identify and protect these nerve branches
. They often lie directly beneath the subcutaneous fat or within the superficial fascial layers. Undermine the skin edges only enough to facilitate clear visualization, using fine hooks or blunt dissection to isolate the nerves.
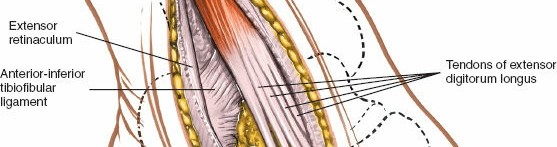
and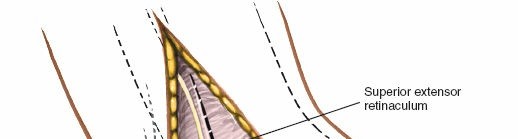highlight the superficial dissection and nerve identification. - Superficial Veins : Small superficial veins crossing the incision should be identified, ligated, or carefully cauterized to prevent post-operative hematoma formation.
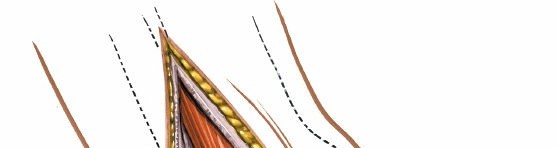
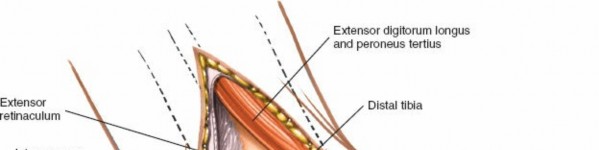
3. Deep Fascia and Internervous Plane
- Incise Deep Fascia : After protecting the superficial peroneal nerve branches, incise the deep fascia longitudinally, parallel to the anterior border of the fibula.
- Identify Internervous Plane : The internervous plane is located between the peroneal muscle belly/tendons (peroneus longus and brevis, supplied by the superficial peroneal nerve) posteriorly and the anterior compartment muscles (extensor digitorum longus, peroneus tertius, supplied by the deep peroneal nerve) anteriorly.
-
Muscle Retraction
: Retract the anterior compartment muscles (EDL, PT) anteriorly and medially. Retract the peroneal tendons (PL, PB) posteriorly. This creates a safe corridor to the underlying bone.
anddemonstrate the exposure of this plane. This plane leads directly to the anterior aspect of the distal fibula, the lateral aspect of the distal tibia, and the neck and body of the talus.
4. Deep Surgical Dissection and Exposure
- Periosteal Incision : Incise the periosteum along the anterior border of the fibula, if necessary, and elevate it to expose the bone.
- Ankle Joint Capsule : Incise the anterior and lateral ankle joint capsule to expose the talar dome and distal tibial plafond. This provides direct access for visualization of articular surfaces and reduction of fractures.
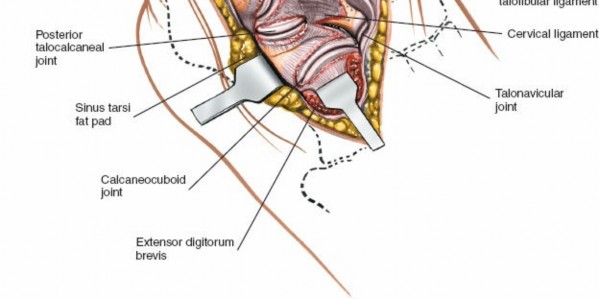
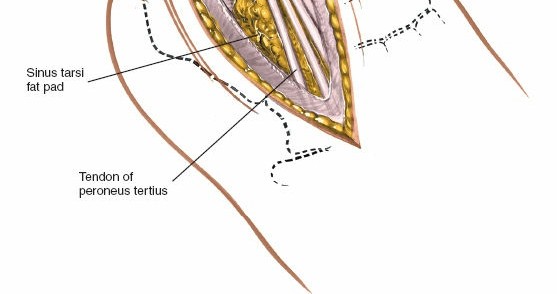
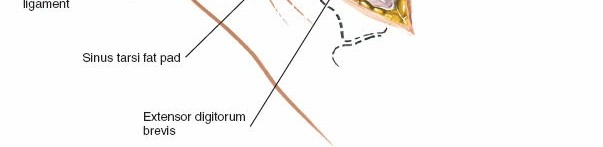
-
Extensor Digitorum Brevis (EDB)
: The EDB muscle originates from the anterior superior aspect of the calcaneus, crosses the sinus tarsi, and lies distal to the ankle joint. To access the lateral aspect of the talus, sinus tarsi, or subtalar joint, the EDB often needs to be detached from its origin and reflected distally or posteriorly.
and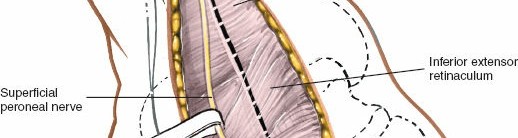illustrate the EDB muscle and its reflection. - Lateral Tarsal Artery : As mentioned in the seed content, the lateral tarsal artery, a branch of the dorsalis pedis artery, frequently crosses the surgical field, especially near the origin of the EDB. It will often be encountered and may need to be ligated or cauterized (diathermy) to prevent the formation of a postoperative hematoma . This step is crucial for maintaining a dry field.
-
Exposure of Bony Structures
:
- Lateral Malleolus/Distal Fibula : Direct access for plating or screw fixation of lateral malleolar fractures.
-
Distal Tibia
: Direct visualization of the anterior inferior tibiofibular ligament (AITFL) for syndesmotic reduction and fixation (
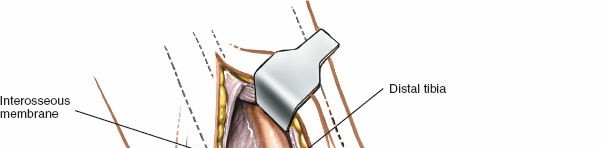). Access to anterolateral pilon fractures. -
Talus
: Excellent visualization of the talar neck and body for fracture reduction and internal fixation (
). Also, allows access for osteochondral lesion procedures. -
Subtalar Joint
: Further dissection inferiorly after EDB reflection provides exposure to the sinus tarsi and lateral aspect of the subtalar joint.
shows a deeper exposure for subtalar visualization. -
Calcaneus/Cuboid
: Can be accessed for anterior process calcaneal fractures or lateral column injuries (
).
5. Reduction and Fixation
- Fracture Reduction : Utilize appropriate reduction clamps, K-wires as joysticks, and periosteal elevators to achieve anatomical reduction of fracture fragments. Restore articular congruity under direct visualization and fluoroscopic guidance.
- Internal Fixation : Apply standard internal fixation techniques, including K-wires, interfragmentary screws, and plates (e.g., one-third tubular, L-plates, contoured anatomical plates) as dictated by the fracture pattern and surgeon's preference. For syndesmotic injuries, use appropriate reduction clamps and screws (cortical or syndesmotic screws).
- Ligament Repair/Reconstruction : For lateral ankle instability, the ATFL and CFL can be repaired directly or reconstructed using various techniques and anchor fixation.
6. Closure
- Irrigation : Copiously irrigate the wound with sterile saline.
- Reapproximation of EDB : If detached, the extensor digitorum brevis muscle can be reattached to its origin using absorbable sutures.
- Deep Fascia Closure : Close the deep fascia over the anterior compartment and peroneal tendons, ensuring no nerve entrapment.
- Subcutaneous Closure : Close the subcutaneous tissue with absorbable sutures to obliterate dead space.
- Skin Closure : Close the skin with non-absorbable sutures or staples.
-
Dressing and Immobilization
: Apply a sterile dressing, followed by a well-padded splint (e.g., posterior splint with lateral stirrup) or cast, in a neutral or slightly dorsiflexed position, depending on the procedure and desired immobilization.
depicts final skin closure.
Complications & Management
Despite meticulous technique, complications can arise following the anterolateral approach. Vigilant identification and appropriate management are crucial.
| Complication | Incidence (Approx.) | Salvage Strategies |
|
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE)
| 1-5% (DVT), <1% (PE) | - Prophylactic strategies (mechanical and pharmacologic) are crucial. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is pivotal for optimizing patient outcomes and facilitating a safe return to prior activity levels. Protocols are tailored to the specific pathology treated (e.g., fracture type, ligament repair, arthrodesis, debridement) and patient factors, but general phases can be outlined.
Phase 1: Protective & Inflammatory (0-2 Weeks Post-Op)
- Goals : Protect surgical repair/fixation, manage pain and swelling, promote wound healing.
- Weight-Bearing : Typically non-weight bearing (NWB) on the affected extremity, usually with crutches or knee scooter.
- Immobilization : Maintained in a splint (e.g., posterior splint with lateral stirrup) or cast for optimal stabilization.
- Exercises : Gentle ankle dorsiflexion/plantarflexion within pain-free limits (if allowed by surgeon), toe curls, hip/knee ROM exercises to prevent stiffness in adjacent joints.
- Interventions : Ice, elevation, compression, pain medication. Strict wound care.
Phase 2: Early Motion & Controlled Loading (2-6 Weeks Post-Op)
- Goals : Gradually restore pain-free range of motion, begin protected weight-bearing, minimize muscle atrophy.
- Weight-Bearing : Progress from NWB to partial weight-bearing (PWB) in a controlled ankle motion (CAM) boot or brace, as tolerated and based on radiographic evidence of healing.
- Immobilization : Transition to a CAM boot or hinged ankle-foot orthosis (AFO) which can be removed for exercises.
- Exercises : Active and passive ankle ROM exercises (dorsiflexion, plantarflexion, inversion, eversion) as permitted. Gentle isometric contractions of ankle musculature (dorsiflexors, plantarflexors, invertors, evertors). Stationary bike with low resistance (non-weight bearing or protected).
- Interventions : Continue modalities for pain/swelling. Scar tissue mobilization once wound is fully healed.
Phase 3: Strengthening & Proprioception (6-12 Weeks Post-Op)
- Goals : Restore full ankle ROM, improve strength, enhance proprioception and balance.
- Weight-Bearing : Progress to full weight-bearing (FWB) in the CAM boot/brace, then gradually wean off the boot/brace as strength and stability improve.
- Exercises : Progressive resistive exercises (e.g., resistance bands, light weights for dorsiflexion, plantarflexion, inversion, eversion). Calf raises (bilateral to unilateral). Balance and proprioceptive training (single leg stance, wobble board, uneven surfaces). Gait training emphasizing normal heel-toe progression.
- Interventions : Continue scar management. Begin light functional activities.
Phase 4: Return to Activity & Sport-Specific Training (12+ Weeks Post-Op)
- Goals : Achieve maximal functional capacity, return to work/sport, prevent re-injury.
- Weight-Bearing : Full unassisted weight-bearing.
- Exercises : Advanced strengthening (plyometrics, agility drills, sport-specific movements). Running progression (if appropriate). Jumping and landing mechanics. Continue proprioceptive and balance training.
- Interventions : Gradual return to desired activities, with close monitoring for pain or swelling. Education on injury prevention strategies, including bracing or taping for high-risk activities. Return to full unrestricted activity is highly variable, often taking 4-6 months, and up to a year for high-demand athletes following complex reconstructions or fusions.
Specific Considerations
- Arthrodesis : Weight-bearing progression is strictly guided by radiographic evidence of fusion.
- Ligament Reconstruction : Early controlled motion is often emphasized, but protection from inversion stress.
- OCLTs : Weight-bearing status is critical to allow cartilage healing or graft incorporation.
Summary of Key Literature / Guidelines
The anterolateral approach, while fundamental, continues to be refined with advancements in imaging, instrumentation, and understanding of biomechanics.
- Anatomical Studies : Detailed cadaveric studies (e.g., those by Sarrafian, Hertel, Ebraheim) have precisely mapped the course of the superficial peroneal nerve branches, providing critical guidelines for incision placement and safe dissection. These studies consistently emphasize the variability of the nerve's exit point from the deep fascia and the importance of blunt dissection in superficial layers.
- Ankle Fractures : Meta-analyses and randomized controlled trials consistently demonstrate superior outcomes for displaced, unstable ankle fractures treated with open reduction and internal fixation compared to non-operative management. The anterolateral approach is the cornerstone for addressing lateral malleolus fractures and anterior syndesmotic pathology. Guidelines from organizations like the Orthopaedic Trauma Association (OTA) and AAOS advocate for anatomical reduction and stable fixation, which is readily achievable via this approach. Recent literature explores the utility of minimally invasive plate osteosynthesis (MIPO) techniques through smaller anterolateral incisions for certain fibular fracture patterns, aiming to reduce soft tissue complications.
- Talar Fractures : Outcomes for talar neck and body fractures are directly correlated with the quality of anatomical reduction and stable fixation. Studies by Hawkins, Canale and Kelly, and subsequent authors underscore the high risk of avascular necrosis (AVN) with increasing displacement. The anterolateral approach, often combined with a medial approach for more complex patterns, provides essential exposure for meticulous reduction and fixation, particularly for anterolateral comminution.
- Osteochondral Lesions of the Talus (OCLTs) : For symptomatic OCLTs, especially those on the lateral talar dome, the anterolateral approach allows direct visualization for debridement, microfracture, or osteochondral grafting (OATS/osteochondral allograft transplantation). Current guidelines suggest a trial of non-operative management, but surgical intervention is indicated for persistent symptoms or larger, unstable lesions. Advances in arthroscopic techniques have provided alternative minimally invasive options, but the open anterolateral approach remains a robust option for lesions requiring direct visualization and more extensive intervention.
- Lateral Ankle Instability : The modified Broström-Gould procedure, often performed via an anterolateral approach, is a widely accepted and highly effective technique for chronic lateral ankle instability. Literature supports its efficacy, with good to excellent outcomes reported in 85-95% of patients. Comparative studies with anatomical reconstructions using grafts show similar stability with potentially faster recovery for direct repair.
- Arthrodesis : For tibiotalar or subtalar arthrodesis, the anterolateral approach provides excellent joint access for debridement of cartilage, correction of deformity, and placement of fixation. Outcome studies for ankle and subtalar fusions generally report high rates of union, although complications like malunion or nonunion can occur.
In conclusion, the anterolateral approach to the ankle and hindpart remains a versatile and essential tool in the orthopedic surgeon's armamentarium. A comprehensive understanding of its anatomical basis, meticulous surgical technique, and diligent post-operative care are paramount for achieving optimal patient outcomes across a diverse range of foot and ankle pathologies.
Clinical & Radiographic Imaging