INTRODUCTION TO ANTERIOR TARSAL TUNNEL SYNDROME
Anterior tarsal tunnel syndrome (ATTS) is a relatively uncommon but clinically significant entrapment neuropathy characterized by the compression of the deep peroneal nerve (DPN) as it passes beneath the inferior extensor retinaculum of the foot. First described by Marinacci in 1968, this condition is the dorsal analogue to the more widely recognized medial tarsal tunnel syndrome.
Because the deep peroneal nerve bifurcates into a medial sensory branch and a lateral motor branch near the ankle joint, entrapment can yield a mixed clinical picture of sensory deficits (dysesthesias in the first web space) and motor dysfunction (weakness or atrophy of the extensor digitorum brevis). For the practicing orthopedic surgeon, mastering the anatomical nuances, diagnostic criteria, and surgical decompression techniques for ATTS is essential for resolving chronic dorsal midfoot pain and restoring optimal biomechanical function.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of the dorsal neurovascular anatomy is paramount for safe and effective surgical intervention.
The Extensor Retinacular System
The deep peroneal nerve descends through the anterior compartment of the leg, lying on the interosseous membrane. As it approaches the ankle, it passes deep to the superior extensor retinaculum and subsequently beneath the inferior extensor retinaculum (often termed the cruciate crural ligament).
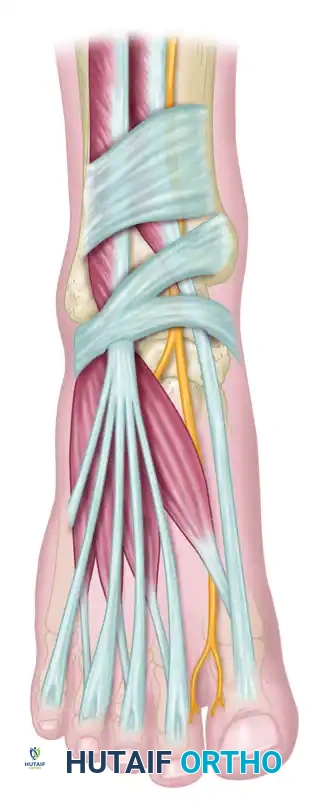
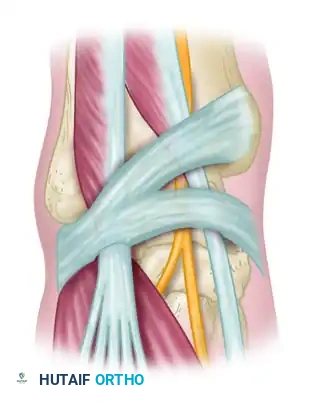

The inferior extensor retinaculum is a Y-shaped band of deep fascia. Its stem attaches laterally to the upper surface of the calcaneus. As it courses medially, it splits into an upper band (attaching to the medial malleolus) and a lower band (blending with the plantar aponeurosis). The deep peroneal nerve and the dorsalis pedis artery travel together within this tight fibro-osseous tunnel, bordered by the tendons of the extensor hallucis longus (EHL) medially and the extensor digitorum longus (EDL) laterally.
Nerve Bifurcation
Just distal to the ankle joint, typically under the proximal edge of the inferior extensor retinaculum, the deep peroneal nerve divides:
1. Medial Terminal Branch (Sensory): Courses alongside the dorsalis pedis artery to provide sensation to the adjacent sides of the first and second toes (the first web space).
2. Lateral Terminal Branch (Motor): Passes deep to the extensor digitorum brevis (EDB) and extensor hallucis brevis (EHB) muscles, providing their motor innervation.
Clinical Pearl: If the motor branch of the deep peroneal nerve arises more proximally than normal (i.e., proximal to the inferior extensor retinaculum), it may escape entrapment, resulting in purely sensory symptoms. Conversely, isolated motor branch entrapment can occur if compression is localized laterally.
ETIOLOGY AND PATHOGENESIS
The pathophysiology of ATTS involves either a decrease in the volume of the anterior tarsal tunnel or an increase in the volume of its contents. Mann and Baxter have extensively documented that this syndrome most commonly occurs due to a combination of biomechanical overload and anatomical impingement.
Extrinsic Compression
- Footwear: Tight-fitting shoes, rigid ski boots, or tightly laced running shoes (especially if a key or timing chip is tied into the laces directly over the retinaculum).
- Repetitive Trauma: Activities that cause repetitive forced plantarflexion or direct dorsal pressure, such as hooking the feet under a bar or bench when performing sit-ups.
Intrinsic Compression
- Osteophytes: Dorsal osteophytes at the anterior ankle joint (tibiotalar), midtarsal (talonavicular), or metatarsocuneiform articulations are the most frequent intrinsic causes. These bony prominences tent the nerve against the unyielding retinaculum.
- Space-Occupying Lesions: Ganglion cysts, tenosynovitis of the extensor tendons, or peripheral nerve sheath tumors.

The circles in the diagram above denote the most common anatomical areas of deep peroneal nerve impingement, highlighting the critical zones over the talonavicular and metatarsocuneiform joints.
CLINICAL EVALUATION
History and Physical Examination
Patients typically present with a vague, deep aching pain over the dorsum of the midfoot that radiates distally into the first web space. Proximally radiating dysesthesias into the anterior compartment of the leg (Valleix phenomenon) may also occur.
Key Physical Findings:
* Sensory Deficit: Decreased light touch and pinprick sensation strictly isolated to the first web space. Sensation should always be compared with the contralateral, asymptomatic foot.
* Tinel's Sign: A positive percussion test over the deep peroneal nerve beneath the inferior extensor retinaculum.
* Motor Deficit: Atrophy or weakness of the EDB muscle. This is assessed by asking the patient to actively extend the toes against resistance while palpating the muscle belly on the lateral dorsum of the foot.
Surgical Warning: If bilateral anterior tarsal tunnel syndrome is present, the surgeon must maintain a high index of suspicion for a diffuse systemic peripheral neuropathy (e.g., diabetic neuropathy, Charcot-Marie-Tooth disease) rather than an isolated mechanical entrapment.
Electrodiagnostic Studies
Electromyography (EMG) and Nerve Conduction Velocity (NCV) studies are the gold standard for confirming the diagnosis.
* EMG Findings: Fibrillations, positive sharp waves, and reduced motor action potentials in the extensor digitorum brevis.
* NCV Findings: Increased distal motor and sensory latencies across the ankle. Crucially, the nerve conduction velocity of the deep peroneal nerve from the fibular neck to the ankle will be normal, ruling out proximal entrapment (e.g., common peroneal nerve entrapment at the fibular head).
DIFFERENTIAL DIAGNOSIS: RELATED NERVE ENTRAPMENTS
When evaluating foot and ankle pain, ATTS must be differentiated from other regional entrapment neuropathies. Understanding the surgical anatomy of these concurrent conditions is vital for accurate diagnosis.
1. Medial Tarsal Tunnel Syndrome (Posterior Tibial Nerve)
Unlike ATTS, medial tarsal tunnel syndrome involves the posterior tibial nerve as it passes beneath the flexor retinaculum (laciniate ligament) on the medial aspect of the ankle. Symptoms typically involve the plantar aspect of the foot.
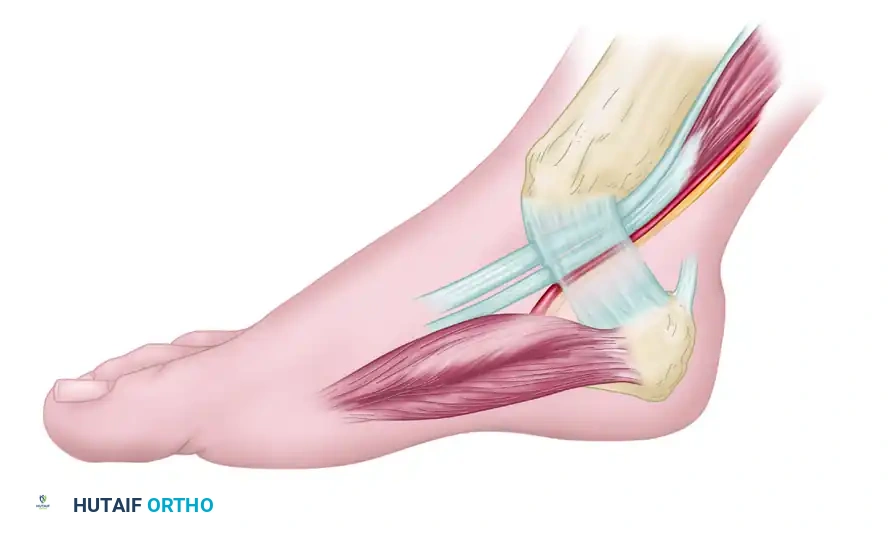
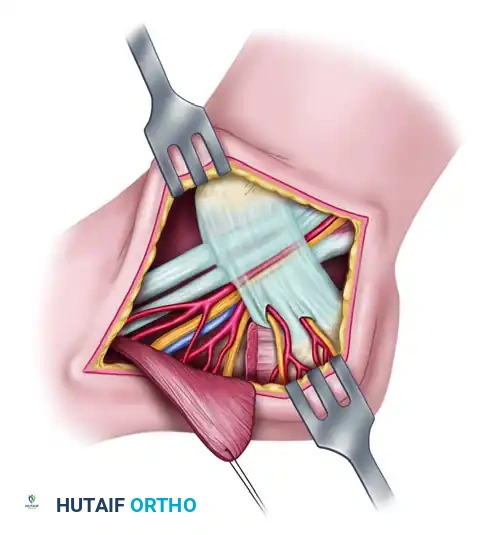
The images above illustrate the standard medial tarsal tunnel release. Note the incision for reflecting the abductor hallucis muscle and the branches of the medial calcaneal nerve and artery penetrating the retinaculum. While anatomically distinct from the anterior tarsal tunnel, the principles of retinacular release and meticulous neurolysis remain identical.
2. Interdigital Neuroma (Morton's Neuroma)
Pain radiating to the toes can also be caused by an interdigital neuroma, most commonly located in the third web space. Unlike the dorsal sensory loss of ATTS, a neuroma presents with plantar pain, a positive Mulder's click, and sensory changes in the adjacent plantar aspects of the toes.
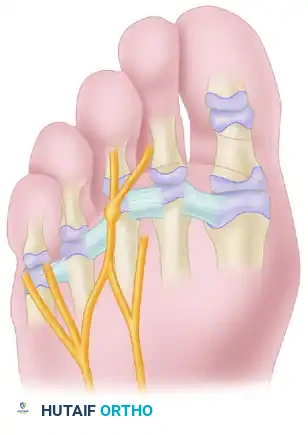
Most common anatomical location of an interdigital neuroma, occurring distal to the transverse metatarsal ligament.
NONOPERATIVE MANAGEMENT
Conservative treatment should be exhausted before considering surgical intervention, typically for a period of 3 to 6 months.
* Footwear Modification: Eliminating tight shoes, loosening laces, and avoiding rigid boots.
* Immobilization: A short-leg walking cast or CAM boot to reduce mechanical irritation.
* Pharmacotherapy: NSAIDs and neuropathic pain modulators (e.g., gabapentin, pregabalin).
* Corticosteroid Injections: An ultrasound-guided injection of local anesthetic and corticosteroid beneath the inferior extensor retinaculum can be both diagnostic and therapeutic.
SURGICAL MANAGEMENT: OPERATIVE TECHNIQUE
Operative decompression and neurolysis of the deep peroneal nerve distal to the ankle joint are indicated when nonoperative measures fail, or if there is progressive motor atrophy of the EDB.
Positioning and Preparation
- The patient is placed in the supine position.
- A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position.
- A thigh tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying delicate nerve fascicles and small crossing vessels.
- Standard orthopedic skin preparation and draping are performed.
Step-by-Step Surgical Approach
1. Incision and Superficial Dissection
- A 4 to 5 cm longitudinal dorsal incision is made over the anterior ankle and midfoot, centered over the area of maximal Tinel's sign or palpable osteophyte. The incision is typically placed just lateral to the extensor hallucis longus (EHL) tendon.
- Meticulous blunt dissection is used in the subcutaneous tissues to identify and protect the branches of the superficial peroneal nerve, which cross the surgical field from lateral to medial.
2. Retinacular Release
- The inferior extensor retinaculum is identified.
- Using a Freer elevator, the surgeon carefully separates the retinaculum from the underlying deep peroneal nerve and dorsalis pedis artery.
- The retinaculum is sharply divided longitudinally. It is crucial to release both the superior and inferior limbs of the Y-shaped ligament to ensure complete decompression.
3. Deep Peroneal Neurolysis
- The deep peroneal nerve is identified and traced distally to its bifurcation.
- If the nerve is encased in dense scar tissue (epineural fibrosis), a careful external neurolysis is performed using micro-scissors and loupe magnification.
- The motor branch is traced laterally under the EDB muscle belly to ensure no secondary crush points exist.
4. Addressing Bony Pathology (Osteophytes)
- If a dorsal osteophyte (e.g., talonavicular exostosis) is the source of impingement, the nerve and artery are gently retracted using vessel loops.
- The periosteum over the osteophyte is incised, and the bony prominence is resected flush with the native cortex using a rongeur or an oscillating saw.
- Bone wax may be applied to the raw cancellous surface to minimize postoperative bleeding and hematoma formation, which could lead to recurrent nerve tethering.
Addressing Space-Occupying Lesions
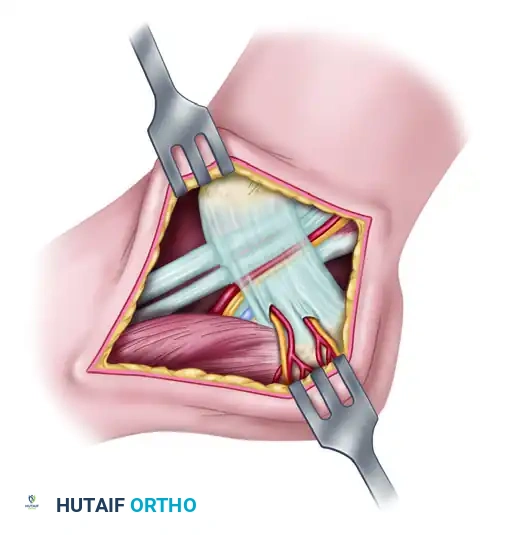
In cases where a ganglion cyst or a peripheral nerve sheath tumor (e.g., schwannoma) is identified within the tunnel, meticulous microsurgical resection is required. The principles of nerve-sparing tumor resection in the foot are universal, whether dealing with the deep peroneal nerve dorsally or the posterior tibial nerve medially.

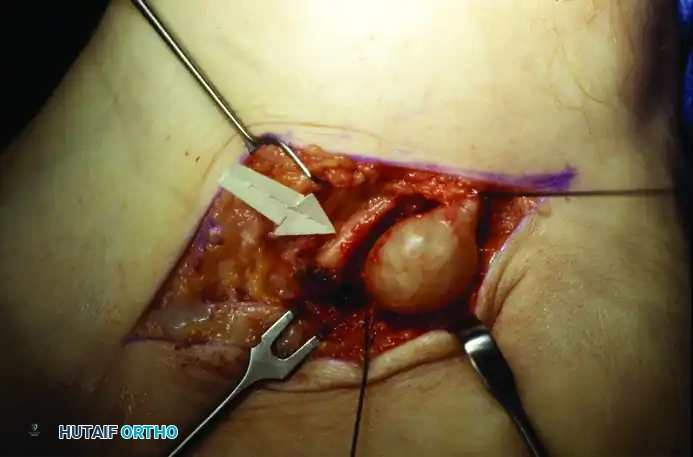
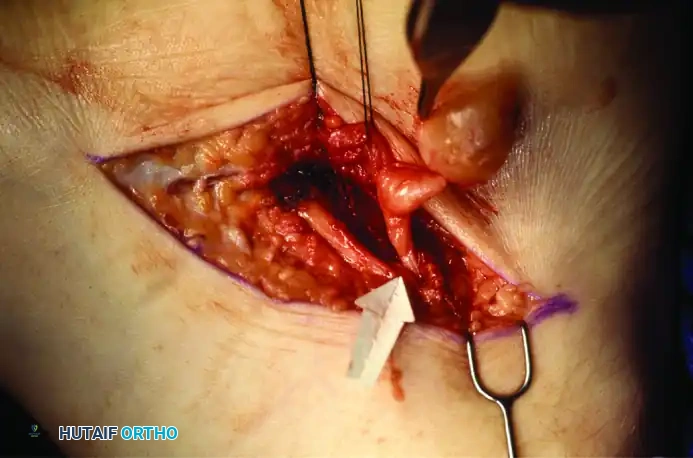
The intraoperative sequence above demonstrates the meticulous resection of a space-occupying lesion. In this analogous example, a tumor involves the medial calcaneal branch of the nerve. Through careful micro-dissection, the tumor was completely resectable while leaving the majority of the nerve branch intact. This exact principle of fascicular preservation must be applied when excising ganglion cysts or tumors compressing the deep peroneal nerve in the anterior tarsal tunnel.
Closure
- The tourniquet is deflated prior to closure to achieve meticulous hemostasis. Hematoma prevention is critical to avoid postoperative scarring around the nerve.
- The inferior extensor retinaculum is left open to prevent recurrent compression.
- The subcutaneous tissue is closed with absorbable sutures, and the skin is closed with non-absorbable monofilament or subcuticular sutures.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative recovery following anterior tarsal tunnel release requires a balance between protecting the surgical site and preventing perineural adhesions.
Phase I: Immediate Postoperative (Weeks 0-2)
- The foot is placed in a bulky, non-compressive Jones dressing and a posterior splint in neutral dorsiflexion.
- Strict non-weight-bearing (NWB) status is maintained to allow the skin to heal and prevent mechanical stress on the decompressed nerve.
- Elevation of the limb is mandated to minimize edema. As noted in the literature, persistent edema for many weeks is common if the dissection has been extensive.
Phase II: Early Mobilization (Weeks 2-6)
- Sutures are removed at 14 days.
- The patient is transitioned to a controlled ankle motion (CAM) boot.
- Progressive weight-bearing is initiated as tolerated.
- Active and active-assisted range of motion (ROM) exercises for the toes and ankle are begun to promote nerve gliding and prevent tethering within the surgical bed.
Phase III: Strengthening and Return to Activity (Weeks 6-12+)
- Transition to standard, wide-toe-box footwear.
- Physical therapy focuses on strengthening the anterior compartment musculature, particularly the EDB and EHL.
- Proprioceptive training and gradual return to high-impact activities (e.g., running) are permitted once the patient is pain-free and demonstrates symmetrical strength.
Clinical Pearl: Patients must be counseled preoperatively regarding the timeline for nerve recovery. While pain relief may be immediate, the resolution of dysesthesias and the return of motor function (if EDB atrophy was present) can be protracted. Complete neurological recovery may require 6 to 12 months, depending on the chronicity and severity of the preoperative compression.
COMPLICATIONS AND PITFALLS
While surgical decompression of the anterior tarsal tunnel is generally highly successful, surgeons must be vigilant to avoid specific complications:
- Iatrogenic Nerve Injury: The superficial peroneal nerve branches are highly vulnerable during the initial skin incision. Injury can result in painful neuroma formation, which is often more debilitating than the original pathology.
- Incomplete Release: Failure to fully divide the distal extensions of the inferior extensor retinaculum can lead to persistent symptoms.
- Recurrent Entrapment: Inadequate hemostasis leading to hematoma, or failure to resect an underlying osteophyte, can cause recurrent scarring and tethering of the deep peroneal nerve.
- Vascular Injury: The dorsalis pedis artery is intimately associated with the nerve. Careless dissection can lead to arterial laceration or pseudoaneurysm formation.
By adhering to strict anatomical principles, utilizing appropriate magnification, and ensuring complete release of all compressive structures, the orthopedic surgeon can reliably restore function and eliminate pain in patients suffering from anterior tarsal tunnel syndrome.
