Anterior Retroperitoneal Approach: Step-by-Step for Lumbar Spine Surgery
Introduction & Epidemiology
The anterior retroperitoneal approach to the lumbar spine represents a well-established surgical pathway for addressing various pathologies affecting the anterior column. This approach prioritizes direct visualization of the intervertebral disc space, enabling comprehensive discectomy, thorough endplate preparation, restoration of sagittal balance, and the placement of robust interbody support devices. Historically, anterior lumbar interbody fusion (ALIF) emerged as a direct alternative or adjunct to posterior fusion techniques, offering unique biomechanical advantages. Its evolution has been driven by advancements in surgical technique, instrumentation, and imaging, moving from open, often morbid, exposures to less invasive modifications.
Lumbar degenerative disc disease (DDD) is a significant cause of axial low back pain, with a global point prevalence estimated between 7.2% and 15%. When conservative management fails, surgical intervention is often considered. Conditions such as degenerative spondylolisthesis, instability, sagittal imbalance, and post-laminectomy syndrome frequently necessitate anterior column support. The anterior retroperitoneal approach is particularly advantageous for lumbosacral junction pathology (L5/S1) due to the challenging anatomical access posteriorly and the ability to achieve superior lordosis restoration anteriorly. While the incidence of ALIF procedures varies, its utilization remains consistent for specific indications, especially those requiring large interbody footprints and robust anterior support.
Surgical Anatomy & Biomechanics
A profound understanding of the surgical anatomy of the anterior retroperitoneal space and the associated lumbar spine is paramount for safe and effective execution of this approach.
Musculoskeletal Anatomy
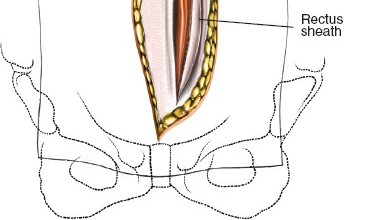
The lumbar spine typically consists of five vertebral bodies (L1-L5) and the sacrum. The intervertebral discs provide cushioning and allow movement. The anterior longitudinal ligament (ALL) runs along the anterior surfaces of the vertebral bodies and discs, providing significant anterior stability. Access to the lumbar spine via the anterior retroperitoneal approach involves navigating through the anterior abdominal wall musculature:
*
Rectus Abdominis:
A paired muscle running vertically, enclosed by the rectus sheath.
*
External Oblique, Internal Oblique, and Transversus Abdominis:
Layers of muscle lateral to the rectus, whose fibers run in different directions, forming the lateral abdominal wall.
Vascular Anatomy
The major vascular structures are the most critical anatomical considerations:
*
Aorta:
Located on the left side of the vertebral column, bifurcating into the common iliac arteries typically at the L4 level.
*
Inferior Vena Cava (IVC):
Located on the right side of the vertebral column, formed by the confluence of the common iliac veins, typically at the L5 level.
*
Common Iliac Arteries and Veins:
Originate from the aorta and IVC, respectively, supplying and draining the lower extremities. These vessels cross anterior to the L5/S1 disc space.
*
Segmental Lumbar Arteries and Veins:
Arise from the aorta and IVC, respectively, supplying the vertebral bodies and paraspinal muscles. These can be encountered during mobilization and often require careful ligation.
*
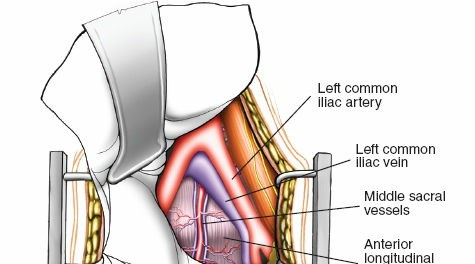
Middle Sacral Artery and Vein:
Typically located anterior to the L5/S1 disc, originating from the distal aorta and draining into the IVC or left common iliac vein, respectively. These often require ligation.
Neural Anatomy
Several critical neural structures are at risk:
*
Lumbar Sympathetic Chain:
Paired ganglia running anterolateral to the vertebral bodies, medial to the psoas muscle. Injury can lead to sympathetic dysfunction, most notably retrograde ejaculation in males (due to injury to the superior hypogastric plexus or direct injury to the sympathetic chain at L5/S1).
*
Genitofemoral Nerve:
Emerging from the psoas muscle, typically crossing the common iliac vessels. It provides sensation to the groin and anterior thigh.
*
Ureters:
Paired tubes carrying urine from the kidneys to the bladder. They descend retroperitoneally, passing over the common iliac vessels. While usually lateral to the operative field, careful identification is essential.
Biomechanics
The anterior column bears approximately 80% of the axial load on the lumbar spine. Interbody fusion through an anterior approach offers several biomechanical advantages:
*
Large Graft Footprint:
Allows for the insertion of large cages or bone grafts, maximizing surface area for fusion and resisting subsidence.
*
Restoration of Disc Height and Lordosis:
Direct access allows for aggressive distraction and placement of lordotic cages, correcting sagittal imbalance and potentially decompressing neural elements indirectly.
*
Load Sharing:
The anterior column provides immediate axial load sharing through the interbody device, reducing stress on posterior instrumentation if used concurrently.
*
Prevention of Pseudoarthrosis:
Enhanced stability and graft contact area contribute to higher fusion rates compared to some posterior-only approaches.
Indications & Contraindications
The anterior retroperitoneal approach is a versatile tool in the orthopedic surgeon's armamentarium, but appropriate patient selection is critical.
Operative Indications
- Degenerative Disc Disease (DDD): Particularly for intractable axial low back pain refractory to extensive conservative management, often associated with disc height loss or instability.
- Degenerative Spondylolisthesis: Especially low-grade (Meyerding Grade I or II) where restoration of disc height and sagittal alignment is beneficial.
- Isthmic Spondylolisthesis: Low-grade slips at L5/S1 can be effectively stabilized and reduced with an ALIF, often combined with posterior fixation.
- Pseudarthrosis / Failed Back Surgery Syndrome (FBSS): Revision surgery for failed posterior fusions, where anterior column support can augment fusion.
- Spinal Deformity Correction: Used to achieve anterior column release, optimize sagittal alignment, and restore lordosis, particularly in cases of flatback syndrome or adult degenerative scoliosis.
- Spinal Infection: For debridement of discitis or osteomyelitis, especially tuberculosis, followed by structural graft placement and fusion.
- Tumor Resection: Resection of anterior column tumors and reconstruction.
- Trauma: Reconstruction of burst fractures or other anterior column instability, though less common than posterior fixation.
- Total Disc Arthroplasty (TDA): The anterior approach is the standard for lumbar disc replacement.
Contraindications
-
Absolute Contraindications:
- Severe Aortoiliac Atherosclerotic Disease: Extensive calcification or aneurysmal disease significantly increases the risk of major vascular injury during vessel mobilization.
- Significant Retroperitoneal Fibrosis: Can obscure anatomical planes and make safe dissection impossible.
- Active Systemic Infection: Increases the risk of surgical site infection.
- Morbid Obesity (Extreme): While not an absolute contraindication, it can significantly increase surgical difficulty, operative time, and complication rates, and may lead to preference for other approaches.
- Limited Access due to Previous Abdominal Surgery: Extensive adhesions from prior open abdominal procedures (e.g., colectomy, appendectomy, gynecological surgery) can make retroperitoneal dissection hazardous.
-
Relative Contraindications:
- Severe Osteopenia/Osteoporosis: May compromise construct stability and increase the risk of implant subsidence.
- Congenital Vascular Anomalies: While sometimes manageable with careful planning (e.g., circumaortic renal vein), can increase risk.
- Extensive Lymphadenopathy: Can obscure the surgical field and necessitate careful dissection to avoid lymphatic injury.
Table of Indications for Anterior Retroperitoneal Lumbar Spine Surgery
| Category | Operative Indications | Non-Operative Considerations (Failure Warrants Surgery) |
|---|---|---|
| Degenerative | Intractable axial low back pain from DDD | Physical therapy, NSAIDs, epidural injections, nerve blocks, activity modification, bracing |
| Degenerative spondylolisthesis (Grade I/II) | ||
| Adjacent segment disease (ASD) following previous fusion | ||
| Deformity | Sagittal imbalance (e.g., flatback syndrome) requiring lordosis restoration | |
| Adult degenerative scoliosis requiring anterior release/support | ||
| Revision Surgery | Pseudarthrosis after previous posterior fusion | |
| Failed Back Surgery Syndrome with clear anterior column pathology | ||
| Infection | Discitis or osteomyelitis requiring debridement and fusion (e.g., spinal tuberculosis) | IV antibiotics (if no instability/neurologic compromise and debridement not immediately indicated) |
| Tumor/Trauma | Anterior column spinal tumors requiring resection and reconstruction | |
| Specific unstable burst fractures of the lumbar spine (less common than posterior for trauma) | ||
| Arthroplasty | Lumbar Total Disc Arthroplasty (for specific indications) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of a successful and safe anterior retroperitoneal lumbar spine surgery.
Pre-Operative Planning
- Comprehensive Clinical Evaluation: Detailed history and physical examination, neurological assessment, and evaluation of pain characteristics.
-
Imaging Review:
- MRI: Essential for assessing neural compression, disc pathology, endplate changes, and spinal cord/nerve root anatomy.
- CT Scan: Provides detailed bony anatomy, assessment of endplate integrity, evaluation of spondylolisthesis reduction, and detection of calcification in great vessels.
- Dynamic X-rays: Flexion/extension views to assess spinal instability.
- CT Angiogram (CTA) or MR Angiogram (MRA): Crucial for mapping the exact course of the great vessels, identifying anomalies (e.g., circumaortic left renal vein, high aortic bifurcation), and assessing atherosclerotic burden, especially if prior abdominal surgery or advanced age are factors. This helps anticipate the required vascular mobilization.
-
Consultations:
- Vascular Surgeon: Often a prerequisite for complex cases, revision surgery, or when significant vascular anomalies or disease are identified. Their presence during the exposure can be invaluable.
- General Surgeon: May be involved if extensive intra-abdominal adhesions are anticipated or if there is concern for bowel injury.
- Blood Management: Type and cross-match blood should be readily available, given the potential for significant vascular injury.
- Patient Education and Consent: Thorough discussion regarding the specific risks associated with the anterior approach, including vascular injury, bowel injury, ureteral injury, and specifically retrograde ejaculation in males, is mandatory.
- Pre-operative Optimization: Addressing medical comorbidities (e.g., diabetes, hypertension, smoking cessation) to optimize patient health status and reduce perioperative risks.
- Surgical Team Briefing: Review of patient specifics, potential challenges, and contingency plans.
Patient Positioning
"Position the patient lying flat and supine on a radiolucent table."
*
Supine Position:
The patient is positioned supine on an operating table specifically designed for fluoroscopic imaging.
*
Padding:
All pressure points (heels, elbows, occiput) should be meticulously padded to prevent pressure sores or nerve palsies.
*
Arm Placement:
Arms are typically tucked at the sides or abducted on arm boards, ensuring intravenous access and careful monitoring.
*
Foley Catheter:
A urinary catheter is inserted to decompress the bladder, which facilitates exposure and minimizes the risk of bladder injury.
*
Gastric Decompression:
An orogastric or nasogastric tube may be considered to decompress the stomach and bowel, particularly in cases where extensive peritoneal mobilization is anticipated.
*
DVT Prophylaxis:
Sequential compression devices (SCDs) are applied to the lower extremities, and chemical prophylaxis is administered per institutional protocol.
*
C-arm Access:
The patient's position must allow for unrestricted movement of the fluoroscopy C-arm to obtain adequate anterior-posterior and lateral views of the lumbar spine for localization and implant assessment.
*
Surgeon and Assistant Positioning:
The primary surgeon typically stands on the side of the incision (usually the patient's left for L5/S1 to follow the natural curve of the vessels, or right for higher levels to displace the IVC). A vascular surgeon or assisting surgeon may be positioned opposite.
Detailed Surgical Approach / Technique
The anterior retroperitoneal approach is performed through a careful, layered dissection to access the lumbar spine while protecting vital structures. The choice of incision and specific dissection planes depends on the target level(s).
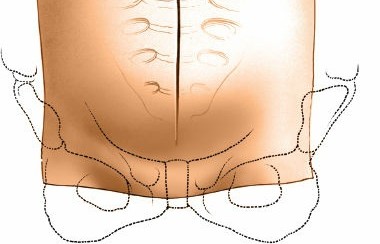
Landmarks and Incisions
The original seed content highlights key landmarks: "The landmark for access to the L5-S1 disc is usually distal to the midway mark between the umbilicus and symphysis. This is not directly over the disc space being distal to it. A more distal incision is required for the L5-S1 disc because of its downward orientation. The anterior landmark for the L4-5 disc is generally located a few centimeters from the umbilicus, and the L3-4 landmark is a few centimeters proximal to the umbilicus. The final localization should be done by fluoroscopy prior to the incision as the disc level may vary."
- Fluoroscopic Localization: Prior to incision, confirm the precise disc level(s) using fluoroscopy. A sterile radio-opaque marker (e.g., needle, Kocher clamp) is placed on the skin, and AP and lateral images are obtained to project the desired disc space onto the abdominal wall.
-
Incision Type:
- Transverse/Oblique Incision: Most commonly used, especially for L5/S1. A slightly oblique Pfannenstiel-type incision or a left-sided oblique incision (often from lateral to medial, superior to inferior) provides excellent cosmetic results and adequate exposure.
- Paramedian Incision: A vertical incision, typically left paramedian, can be used, particularly for multilevel fusion or when broader exposure is needed.
Step-by-Step Dissection
-
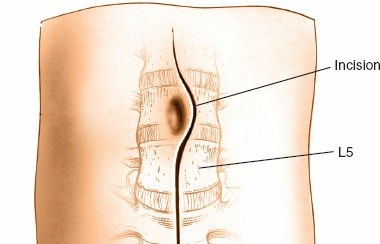
Skin Incision and Subcutaneous Dissection:
- Once the desired level is confirmed by fluoroscopy, a sterile marking pen is used to delineate the incision.
- The skin is incised with a scalpel.
- Subcutaneous tissue is divided using electrocautery, maintaining meticulous hemostasis.
- The incision is deepened to the level of the anterior rectus sheath.

-
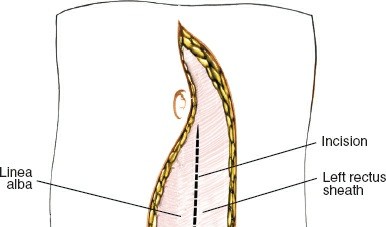
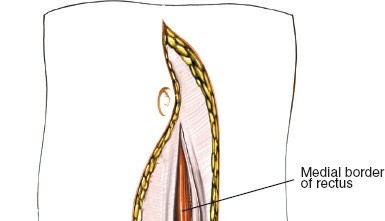
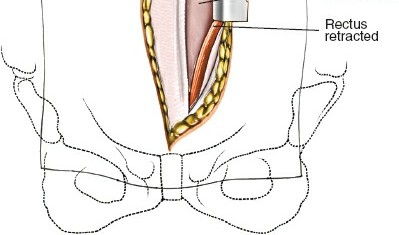
Anterior Fascial Layers & Rectus Sheath:
- The anterior rectus sheath is identified. For a left-sided approach, the sheath is incised longitudinally, typically just medial to the rectus abdominis muscle, or the muscle itself is retracted laterally.
- Alternatively, for a paramedian approach, the rectus abdominis is identified and retracted medially (often preferred to avoid rectus splitting which can denervate the medial portion). If a muscle-splitting approach is utilized, the rectus fibers are carefully separated in the direction of their fibers.
-
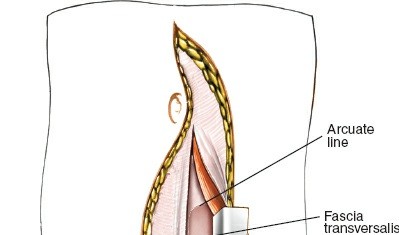
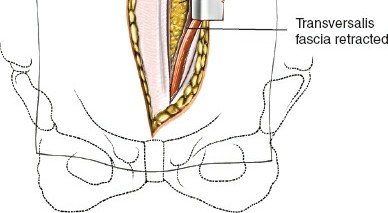
Internervous Plane / Retroperitoneal Entry:
- The original seed mentions "An interval just medial to the rectus abdominis and under th". This refers to the plane beneath the rectus abdominis muscle. After mobilizing or splitting the rectus, the posterior rectus sheath and transversalis fascia are incised.
- Careful blunt dissection is then performed, gently sweeping the peritoneum and its contents (bowel) medially and to the right, using a combination of fingers and sponges. The aim is to remain entirely retroperitoneal, avoiding entry into the peritoneal cavity. This plane is relatively avascular.
-
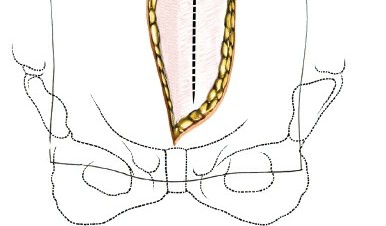
Peritoneal Reflection and Retroperitoneal Space Entry:
- As the peritoneum is reflected medially, the psoas muscle is typically identified laterally, serving as a landmark for the retroperitoneal space.
- The dissection continues until the major vascular structures (aorta and IVC) are encountered, lying anterior to the vertebral column.
- Self-retaining retractors (e.g., Bookwalter, Omni-Tract) are carefully placed to maintain exposure, ensuring that the blades retract the peritoneum and its contents without causing injury.
-
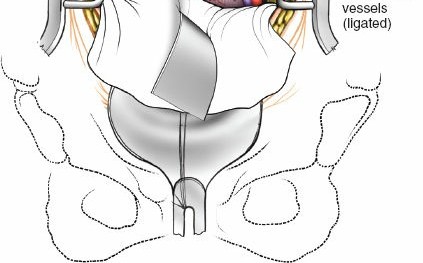
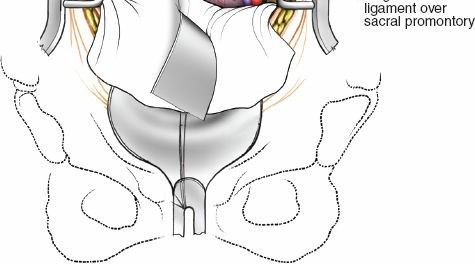
Vascular Identification & Mobilization:
- The great vessels (aorta on the left, IVC on the right) are meticulously identified. The common iliac arteries and veins are also visualized, especially for L5/S1 exposure where they cross the disc space.
- The lymphatic plexus lying anterior to the vessels should be carefully swept off the vessel walls. Extensive injury to these lymphatics can lead to lymphocele formation postoperatively.
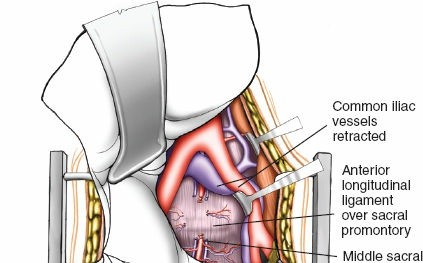
- The vessels are then gently mobilized to expose the anterior aspect of the disc space. For L5/S1, the left common iliac vein is typically retracted to the left, and the right common iliac artery and vein are retracted to the right. This often requires careful ligation of the middle sacral vessels (artery and vein) and sometimes segmental lumbar vessels.
- Ligation of vessels should be performed with fine sutures (e.g., 4-0 or 5-0 prolene) or clips, ensuring secure hemostasis. The vascular surgeon often performs this step.

-
Exposure of Anterior Lumbar Spine:
- Once the vessels are safely mobilized, the anterior longitudinal ligament (ALL) covering the disc space and vertebral bodies is clearly visible.
- Specific ALIF retractors with thin blades designed to protect the great vessels and sympathetic chain are then strategically placed. These blades are inserted into the retroperitoneal space, gently retracting the vessels and adjacent soft tissues. Careful attention is paid to the depth and angle of retraction to prevent injury.
-
Discectomy and Endplate Preparation:
- The ALL is incised over the target disc space.
- A complete discectomy is performed using scalpels, rongeurs, pituitary curettes, and curettes. All disc material, including the annulus and nucleus pulposus, must be removed to facilitate fusion.
- The cartilaginous endplates are meticulously removed down to bleeding subchondral bone, preserving the integrity of the cortical endplates. Over-resection can lead to subsidence, while inadequate removal can impede fusion. This step is critical for bone-to-bone contact and fusion.
-
Cage/Graft Insertion:
- Trial sizers are used to determine the optimal footprint, height, and lordotic angle of the interbody cage. The goal is to restore disc height, decompress neural elements indirectly, and re-establish sagittal alignment.
- The chosen interbody device (e.g., PEEK cage, titanium cage, allograft, autograft) is packed with bone graft material (autograft, allograft, or synthetic bone substitutes).
- The graft-filled cage is then carefully impacted into the prepared disc space. Ensure proper seating and engagement with the bony endplates.
- For total disc arthroplasty, the prosthesis components are prepared and inserted according to manufacturer specifications.

-
Optional Anterior Plate Fixation:
- In many ALIF constructs, supplemental anterior plating is utilized to enhance immediate construct stability, prevent cage migration, and improve fusion rates, especially for single-level fusions or in cases of instability.
- The plate is contoured to the anterior vertebral bodies and secured with bicortical or unicortical screws, avoiding penetration into the spinal canal or adjacent disc spaces.
-
Closure:
- All retractors are carefully removed, and thorough hemostasis is ensured. Inspect the great vessels for any signs of injury (e.g., hematoma, pulsatile flow disruption) and the peritoneum for tears.
- The mobilized vessels are allowed to fall back into their anatomical position.
- The posterior rectus sheath and transversalis fascia are reapproximated with absorbable sutures.
- The rectus abdominis muscle (if split) or its fascia is closed.
- The anterior rectus sheath is closed with robust absorbable sutures.
- The subcutaneous tissue and skin are closed in layers. A surgical drain is rarely necessary unless significant bleeding or lymphatic ooze is observed.
Complications & Management
Despite its advantages, the anterior retroperitoneal approach carries a unique set of potential complications that require vigilant prevention and prompt management.
Table of Common Complications, Incidence, and Management
| Complication | Incidence (%) | Management / Salvage Strategy |
|---|---|---|
| Vascular Injury | 1-15% (major) | Immediate vascular surgeon consultation. Direct repair with non-absorbable sutures (e.g., Prolene). Hemostasis with pressure, vascular clamps. Potential for graft interposition (e.g., saphenous vein, synthetic). Post-op monitoring for hemorrhage, pseudoaneurysm, AV fistula. Intraoperative mortality possible. |
| Retrograde Ejaculation | 0.5-30% (males) | Primarily preventive: careful blunt dissection of presacral plexus, minimize electrocautery near sympathetic chain, gentle retraction. If transient, monitor. If persistent, counseling, fertility specialist referral. Often due to sympathetic nerve disruption at L5/S1. |
Complications & Management Table
| Category | Incidence (%) | Management / Salvage Strategy |
|
Primary Goal:
| Achieve solid fusion and correction of instability/deformity. |
|
Neural
| | |
| ** |
| | |
| | |
| **V |
| ** |
| | |
| ** | |
| | |
| | |
| ** | |
| ** | |
| ** | |
| | |
| | |
| | |
| | |
| | |
| ** | |
| | |
| | |
| | |
| ** | |
| ** | |
| | |
| ** | |
| ** | |
| ** | |
| ** | |
| ** | |
| ** | |
| ** | |
| ** | |
| ** | |
| |
Clinical & Radiographic Imaging