Comprehensive Introduction and Patho-Epidemiology
Anterior interbody arthrodesis with instrumentation for the correction of adolescent idiopathic scoliosis (AIS) represents one of the most mechanically powerful and biologically sound techniques in the armamentarium of the modern orthopedic spine surgeon. Historically pioneered by Dwyer and later refined by Zielke and Harms, the anterior approach directly addresses the primary site of the scoliotic deformity: the anterior column and the intervertebral disc. By excising the disc spaces, the surgeon effectively releases the anterior tether, allowing for profound mobilization of the spinal column. This masterclass delineates the intricate execution of this procedure, transitioning from foundational preoperative evaluation to the nuanced biomechanics of intraoperative derotation and stabilization. Our overarching objective transcends mere radiographic correction; it is the durable restoration of coronal and sagittal balance, the preservation of motion segments, and the meticulous avoidance of iatrogenic complications.
The pathophysiology of idiopathic scoliosis is inherently three-dimensional, characterized by a complex interplay of coronal translation, sagittal plane alteration (typically hypokyphosis in the thoracic spine), and axial rotation. The apical vertebrae rotate such that the vertebral bodies migrate towards the convexity of the curve, while the posterior elements are driven towards the concavity. This rotational coupling is the primary driver of the clinically apparent rib hump or lumbar prominence. Anterior interbody arthrodesis is uniquely suited to address this specific pathoanatomy. By placing instrumentation directly on the convex lateral aspect of the vertebral bodies, the surgeon applies compressive and derotational forces directly at the apex of the deformity, achieving a true three-dimensional correction that is often biomechanically superior to posterior-only constructs for specific curve patterns.
Epidemiologically, while posterior spinal fusion remains the workhorse for the majority of AIS cases, anterior approaches are specifically indicated for a distinct subset of patients. Thoracolumbar and lumbar curves (Lenke type 5) are the classic indication, as the anterior approach frequently allows for the preservation of one to two distal fusion levels compared to a posterior approach, thereby sparing critical lumbar motion segments and potentially reducing the long-term risk of adjacent segment disease. Furthermore, in the skeletally immature patient with a large thoracic curve, an anterior release and fusion definitively prevent the "crankshaft phenomenon"—a progressive rotational deformity caused by continued anterior spinal growth in the presence of a solid posterior fusion mass.
The evolution of anterior instrumentation—from flexible cables to rigid, dual-rod, dual-screw constructs—has dramatically altered the postoperative landscape. Modern rigid systems provide immediate structural stability, often obviating the need for postoperative bracing and significantly reducing the historical rates of pseudarthrosis and implant failure. However, the procedure demands a profound understanding of visceral, vascular, and neural anatomy, as well as a high degree of technical surgical proficiency. The steep learning curve associated with thoracotomy, retroperitoneal dissection, and anterior spinal instrumentation requires rigorous training and an uncompromising approach to surgical planning and execution.
Detailed Surgical Anatomy and Biomechanics
Mastery of anterior spinal surgery is predicated upon an intimate, three-dimensional understanding of the regional anatomy, particularly the critical vascular and neural structures that intimately relate to the anterior spinal column. In the thoracic spine, the aorta lies slightly to the left of the midline, while the azygos vein and superior vena cava are situated on the right. Consequently, right-sided thoracotomies are generally preferred for right-sided thoracic curves, which constitute the vast majority of idiopathic patterns. The segmental vessels—arteries branching directly from the aorta and veins draining into the azygos/hemiazygos system—course transversely across the waist of each vertebral body. These must be meticulously identified, isolated, and ligated to safely expose the intervertebral discs and the lateral aspect of the vertebral bodies for instrumentation.


The neural anatomy encountered during the anterior approach is equally unforgiving. The sympathetic chain descends vertically along the heads of the ribs in the thoracic spine and along the anterolateral aspect of the vertebral bodies in the lumbar spine. Iatrogenic injury to this chain can result in altered temperature regulation in the ipsilateral lower extremity (a "warm leg") or, more distressingly, Horner's syndrome if injured in the upper thoracic spine. In the thoracolumbar junction, the diaphragm crus must be carefully elevated to expose the L1 and L2 vertebral bodies. Further distally, the psoas major muscle envelops the lateral aspect of the lumbar vertebrae. The lumbar plexus is embedded within the substance of the psoas; therefore, retraction of this muscle must be performed with extreme caution to prevent postoperative neuropraxia, particularly of the genitofemoral or lateral femoral cutaneous nerves.
Biomechanically, the anterior interbody arthrodesis operates on the principle of load sharing and anterior column reconstruction. The intervertebral disc is the primary restraint to spinal mobility. By performing a radical discectomy—removing the annulus fibrosus and the nucleus pulposus down to the posterior longitudinal ligament (PLL)—the surgeon completely destabilizes the motion segment, rendering it highly compliant. This radical release is the biomechanical prerequisite for achieving maximal deformity correction with minimal applied force. Once the discs are excised, structural interbody grafts or cages are inserted. These implants serve a dual purpose: they act as a fulcrum for coronal correction during convex compression and provide immediate structural support to the anterior column, placing the bone graft under compression (Wolff's Law) to optimize the biological environment for arthrodesis.



Furthermore, the placement of the instrumentation is paramount to the biomechanical success of the procedure. Screws must be placed parallel to the endplates and directed transversely across the vertebral body to achieve bicortical purchase. This bicortical fixation is critical for resisting the substantial pull-out forces generated during the derotation and compression maneuvers. In modern dual-rod systems, the anterior rod acts primarily as a compression strut to correct the coronal deformity, while the posterior rod (closer to the spinal canal) aids in derotation and the restoration or maintenance of physiological sagittal alignment. The ability to independently manipulate these two rods provides the surgeon with unparalleled control over the three-dimensional spatial orientation of the instrumented spinal segments.
Exhaustive Indications and Contraindications
The decision to proceed with an anterior interbody arthrodesis rather than a posterior or combined approach requires a nuanced analysis of the patient's specific curve morphology, skeletal maturity, and overall physiological status. While the indications have evolved with the advent of powerful posterior pedicle screw constructs, the anterior approach remains the gold standard for specific, carefully selected clinical scenarios.
| Variable | Anterior Interbody Arthrodesis | Posterior Spinal Fusion |
|---|---|---|
| Primary Indication | Lenke 5 (Thoracolumbar/Lumbar), Hypokyphotic Thoracic | Lenke 1, 2, 3, 4, 6, Hyperkyphotic curves |
| Motion Preservation | Often saves 1-2 distal fusion levels in lumbar curves | Typically requires longer fusion constructs |
| Crankshaft Prevention | Definitive prevention in Risser 0/open triradiate | Requires robust pedicle screw fixation to mitigate |
| Pulmonary Impact | Transient decrease in PFTs due to thoracotomy | Less direct impact on pulmonary mechanics |
| Sagittal Profile | Excellent for creating kyphosis (closing wedge) | Better for correcting hyperkyphosis |
The primary indication for an isolated anterior spinal fusion and instrumentation is the presence of a progressive, structural thoracolumbar or lumbar curve (Lenke type 5). In these patients, the anterior approach consistently allows for the lowest instrumented vertebra (LIV) to be placed one or sometimes two levels proximal to what would be required for a posterior approach. By stopping the fusion at L3 instead of L4, or L4 instead of L5, the surgeon preserves vital lumbar motion segments, significantly mitigating the long-term biomechanical stress on the adjacent uninstrumented discs. A secondary, yet critical, indication is the skeletally immature patient (Risser 0, open triradiate cartilage) presenting with a large thoracic curve. In these cases, anterior discectomy and fusion arrest the anterior growth plates, definitively preventing the crankshaft phenomenon that can occur if only a posterior fusion is performed.




Conversely, absolute contraindications to the anterior approach must be rigorously respected to avoid catastrophic perioperative morbidity. Severe pulmonary dysfunction is a primary contraindication. The necessity of a thoracotomy, single-lung ventilation, and potential chest wall disruption can precipitate acute respiratory failure in patients with preexisting restrictive or obstructive lung disease. Preoperative pulmonary function tests (PFTs) are mandatory; a forced vital capacity (FVC) of less than 40% of predicted is generally considered an absolute contraindication to an open thoracotomy approach. Additionally, patients with severe osteopenia or osteoporosis are poor candidates for anterior instrumentation, as the relatively softer cancellous bone of the anterior vertebral body provides insufficient purchase for the screws, leading to a high risk of implant pull-out during deformity correction.
Relative contraindications include a history of previous thoracotomy or significant pleural disease on the side of the planned approach, as dense pleural adhesions can make mobilization of the lung and exposure of the spine exceptionally treacherous. Furthermore, hyperkyphotic thoracic curves (e.g., Scheuermann's kyphosis) are generally not treated with isolated anterior instrumentation. The anterior approach, utilizing compression across the disc spaces, inherently shortens the anterior column and is highly effective at inducing kyphosis; therefore, it is ideal for the hypokyphotic curves typical of AIS but detrimental in patients with preexisting hyperkyphosis. Finally, curves that extend high into the upper thoracic spine (proximal to T4) are technically challenging to access via a standard thoracotomy and are usually better addressed via a posterior approach.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the absolute cornerstone of a successful anterior interbody arthrodesis. This process begins long before the patient enters the operating theater, requiring a comprehensive synthesis of clinical examination findings, advanced radiographic imaging, and precise surgical templating. The goal is to anticipate every anatomical nuance and potential intraoperative challenge, ensuring a seamless and biologically sound execution of the surgical plan.
Clinical Evaluation and Differential Diagnosis
The preoperative assessment begins with a rigorous history and physical examination. Ascertaining the patient's and family's perception of the deformity is critical, noting asymmetric shoulder elevation, truncal shift, waistline asymmetry, and rib or flank prominence. A detailed pain assessment is mandatory; while mild, mechanically related back pain is common in AIS, severe axial pain, night pain, or radicular symptoms are red flags that necessitate immediate investigation with an MRI of the neural axis to rule out intraspinal pathology such as tumors, syringomyelia, or a tethered cord. Neurologic symptoms, including paresthesias, hyperesthesia, or bowel/bladder dysfunction, are absolute indications for advanced imaging. Physically, the Adams Forward Bend Test remains the gold standard for characterizing the axial-plane deformity. Utilizing a scoliometer, we objectively grade the rotational prominence; a reading exceeding 5-7 degrees indicates a significant rotational component requiring surgical derotation. Furthermore, a thorough dermatological inspection must be performed to identify cutaneous stigmata of dysraphism (hairy patches, dimples, lipomas), which may herald underlying congenital spinal anomalies.
Advanced Imaging and Curve Analysis
Our imaging suite provides the definitive roadmap for the surgical intervention. Standard full-length, standing posteroanterior (PA) and lateral radiographs are foundational. On the PA view, we meticulously measure the coronal plane deformity using the Cobb method, identifying the most tilted superior and inferior end vertebrae. Truncal imbalance is quantified using the Floman method, bisecting the distance between the lateral rib margins and comparing this point to the center sacral vertical line (CSVL). Sagittal balance is assessed on the lateral radiograph by dropping a C7 plumb line relative to the posterior superior corner of S1. Crucially, we evaluate skeletal maturity markers, specifically the Risser sign (grading iliac apophysis ossification from 0 to 5) and the status of the triradiate cartilage, to predict remaining growth potential and the risk of the crankshaft phenomenon.

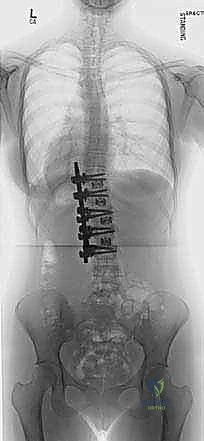
FIG 1A • Preoperative AP radiograph illustrating a 51-degree left lumbar curve, highlighting the coronal plane deformity.

FIG 1B • Preoperative lateral radiograph of the same patient, allowing assessment of sagittal alignment.
Supine best-bend radiographs are indispensable for determining the dynamic flexibility of the spine. These images allow the surgeon to differentiate between primary structural curves and secondary compensatory curves, directly influencing the Lenke classification and the selection of fusion levels. For instance, they dictate whether a compensatory thoracic curve requires inclusion in the fusion construct when addressing a primary thoracolumbar curve. Atypical curve patterns—such as left-sided thoracic curves, short angular curves, or curves associated with excessive kyphosis—mandate an MRI to exclude neurofibromatosis, Marfan syndrome, or Chiari malformations.
Determining Fusion Levels and Templating
The determination of fusion levels is perhaps the most critical cognitive step in the preoperative phase. The general principle dictates fusing from the proximal-end vertebra to the distal-end vertebra. However, the "parallel disc controversy" in thoracic curves requires careful consideration. If a curve is flexible (>50% correction on bend films), relatively small (50-60 degrees), and the patient is skeletally mature, a parallel disc at the distal segment may often be spared. Conversely, in thoracolumbar curves, the disc below the planned lowest instrumented vertebra (LIV) must be scrutinized. If this disc reverses and opens into the fractional lumbosacral curve on the standing radiograph, postoperative wedging is less likely. If it is parallel preoperatively, it will likely wedge postoperatively, potentially leading to global decompensation and necessitating extension of the fusion.
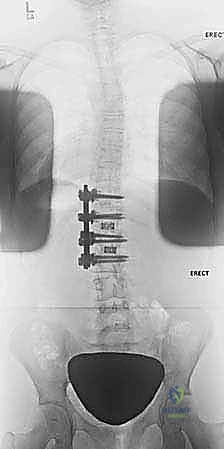
FIG 2A • Preoperative radiograph of a 13-year-old girl with a right thoracic curve measuring 52 degrees from T6 to T12.

FIG 2B • Postoperative thoracoscopic anterior spinal fusion and instrumentation from T6 to T12, showing excellent correction.
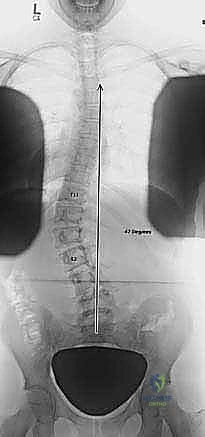
FIG 2C • Preoperative radiograph of a left thoracolumbar curve between T11 and L2 with a trunk shift to the left.
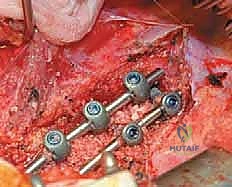
FIG 2D • Two-year postoperative radiographs following an open anterior fusion and instrumentation from T11 to L2.
Preoperative templating utilizes these radiographs to estimate required screw diameters, lengths, and rod contours. Once templating is complete, meticulous patient positioning in the operating room is executed. The patient is placed in the true lateral decubitus position, with the convexity of the curve directed upwards. An axillary roll is placed to protect the dependent brachial plexus, and the patient is securely taped to the operating table to allow for aggressive table tilting during the procedure. Proper positioning is not merely about access; it utilizes gravity to assist in the spontaneous correction of the deformity once the anterior release is performed.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of an anterior interbody arthrodesis is a masterclass in anatomical dissection, aggressive soft-tissue release, and precise biomechanical instrumentation. The procedure demands a seamless orchestration between the orthopedic surgeon, the access surgeon (often a thoracic or general surgeon), and the anesthesia team, particularly regarding the management of single-lung ventilation via a double-lumen endotracheal tube.
Exposure and Vascular Management
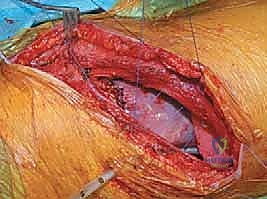
The incision is planned directly over the rib corresponding to the most proximal vertebra to be instrumented, typically following the contour of the rib to optimize cosmetic outcome. For a standard thoracic approach, the periosteum of the selected rib is incised, and the rib is resected subperiosteally. This resected rib will later serve as high-quality autograft for the interbody fusion. The pleural cavity is entered through the rib bed, and the ipsilateral lung is deflated and retracted anteriorly. For thoracolumbar approaches, the diaphragm must be circumferentially detached from its costal insertions, leaving a 1-cm cuff of tissue for later robust repair. The retroperitoneal space is then developed, meticulously reflecting the peritoneal sac and abdominal viscera anteriorly to expose the psoas muscle and the lumbar spine.







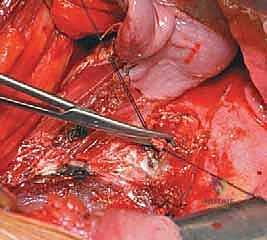
Once the spine is exposed, the segmental vessels must be managed. The parietal pleura is incised longitudinally over the spine. Using blunt dissection, the segmental artery and vein at each level to be fused are isolated at the mid-vertebral body level. These vessels are securely ligated with surgical clips or ties and divided. This mobilization allows the great vessels (aorta and vena cava) to fall away from the spine, providing safe, unobstructed access to the intervertebral discs and the lateral aspect of the vertebral bodies. It is imperative to ligate these vessels at the mid-body level to preserve the collateral blood supply to the spinal cord via the neural foramina.
Radical Discectomy and Endplate Preparation
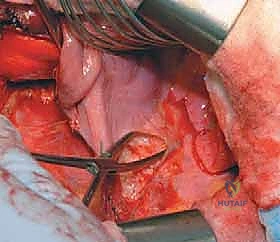
The radical discectomy is the most critical step for achieving both deformity correction and a solid arthrodesis. An annulotomy is performed, and the nucleus pulposus and annulus fibrosus are aggressively excised using a combination of rongeurs, curettes, and Cobb elevators. The dissection must proceed posteriorly to the posterior longitudinal ligament (PLL) and contralaterally to the opposite annulus. Complete excision of the cartilaginous endplates down to bleeding subchondral bone is mandatory. Failure to adequately prepare the endplates is the primary cause of postoperative pseudarthrosis. The thoroughness of this release dictates the flexibility of the spine; a properly released spine will often demonstrate significant spontaneous correction of the deformity merely from patient positioning and gravity.



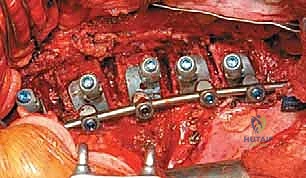
Instrumentation, Derotation, and Fusion
Following the discectomy, structural interbody grafts or titanium/PEEK cages packed with the morselized autologous rib graft are inserted into the anterior third of the disc spaces. These cages act as a fulcrum for correction and restore anterior column height. Next, vertebral body screws are placed. The starting point is typically in the posterior half of the vertebral body to avoid the great vessels. The trajectory must be strictly parallel to the endplates and directed transversely to achieve bicortical purchase on the contralateral cortex. Bicortical fixation is non-negotiable, as it maximizes pull-out strength for the subsequent correction maneuvers.