Introduction & Epidemiology
The tibia, as the largest bone in the lower leg and a critical weight-bearing structure, is highly susceptible to traumatic injury. Tibial shaft fractures constitute the most common long bone fracture, with an incidence rate estimated between 10 to 20 per 100,000 person-years, varying significantly with age, mechanism of injury, and geographic location. These fractures often result from high-energy trauma, leading to extensive soft tissue injury, and can be associated with significant morbidity, including compartment syndrome, infection, nonunion, and chronic pain. The management of tibial fractures and other tibial pathologies demands a profound understanding of surgical anatomy, biomechanics, and various operative approaches.
The anterior approach to the tibia represents a fundamental and versatile surgical corridor, providing direct and comprehensive access to both its medial (subcutaneous) and anterolateral (extensor) surfaces. Historically, this approach has been a cornerstone in orthopedic trauma and reconstructive surgery due to its relative simplicity, extensive exposure capabilities, and predictable anatomical landmarks. Its utility extends beyond acute fracture management to encompass a broad spectrum of elective and emergent conditions, making it an indispensable technique in the orthopedic surgeon's armamentarium. While intramedullary nailing has emerged as the gold standard for most tibial shaft fractures, the anterior approach remains critical for specific fracture patterns, nonunions, tumor excisions, osteomyelitis debridement, and reconstructive procedures where direct visualization and robust plating are paramount. This reference aims to delineate the safe surgical techniques associated with the anterior approach to the tibia, emphasizing meticulous dissection, anatomical preservation, and optimal fixation strategies.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the anatomy of the lower leg is paramount for safely executing the anterior approach to the tibia. The tibia is a prism-shaped long bone with distinct medial, lateral, and posterior surfaces, separated by anterior, interosseous, and posterior borders.
Osteology
The tibial shaft presents a triangular cross-section proximally, becoming more rounded distally. The anterior border is palpable subcutaneously as the "shin." The medial surface is largely subcutaneous along its entire length, particularly in the distal two-thirds. The lateral surface provides attachment for the anterior compartment muscles. The interosseous border serves as the origin for the interosseous membrane, which separates the anterior and posterior compartments and provides attachment for various muscles. The periosteum is a vital structure, contributing significantly to bone healing through its osteogenic potential and vascular supply, especially in younger individuals. The primary vascular supply to the tibial diaphysis is via the nutrient artery , a branch of the posterior tibial artery, which enters the posterior cortex. Additional supply comes from periosteal vessels, particularly important in comminuted fractures where the nutrient artery supply may be disrupted.
Soft Tissue Compartments & Neurovascular Structures
The leg is divided into four distinct fascial compartments by the crural fascia and intermuscular septa:
1.
Anterior Compartment
: Bounded by the tibia, interosseous membrane, anterior intermuscular septum, and deep fascia. Contains the
tibialis anterior
,
extensor hallucis longus (EHL)
,
extensor digitorum longus (EDL)
, and
fibularis tertius
muscles. The
deep fibular nerve
and
anterior tibial artery and veins
run within this compartment, typically on the interosseous membrane or immediately adjacent to it, between the tibialis anterior and EHL/EDL.
2.
Lateral Compartment
: Bounded by the fibula, anterior intermuscular septum, posterior intermuscular septum, and deep fascia. Contains the
fibularis longus
and
brevis
muscles. The
superficial fibular nerve
courses through this compartment, initially deep to the fibularis longus, becoming more superficial in the distal leg, piercing the deep fascia to become subcutaneous.
3.
Superficial Posterior Compartment
: Bounded by the deep fascia and transverse intermuscular septum. Contains the
gastrocnemius
,
soleus
, and
plantaris
muscles.
4.
Deep Posterior Compartment
: Bounded by the interosseous membrane, tibia, fibula, and transverse intermuscular septum. Contains the
tibialis posterior
,
flexor hallucis longus (FHL)
, and
flexor digitorum longus (FDL)
muscles. The
posterior tibial artery and veins
and the
tibial nerve
are also located here.
The saphenous vein and saphenous nerve are superficial structures running subcutaneously along the medial aspect of the tibia. These must be identified and protected during the medial aspect of the approach.
Biomechanics of Plating
The choice between medial (subcutaneous) and anterolateral plating surfaces carries significant biomechanical and soft tissue implications:
-
Medial (Subcutaneous) Surface Plating :
- Biomechanics : The medial aspect of the tibial shaft is considered the tension side during weight-bearing. Applying a plate here aligns with fundamental biomechanical principles of neutralizing tensile forces, particularly beneficial for constructs aiming for absolute stability (e.g., lag screw compression, dynamic compression plating). It is generally easier to contour plates to the relatively flat medial surface.
- Disadvantage : The primary drawback is the sparse soft tissue coverage. Plates placed here are often prominent, leading to increased rates of wound dehiscence, skin irritation, and eventual need for hardware removal. This is particularly problematic in patients with thin skin, compromised vascularity, or following high-energy trauma with significant soft tissue injury.
-
Anterolateral Surface Plating :
- Biomechanics : The anterolateral aspect is considered the compression side during weight-bearing. Plating here places the construct on the convex side of the bending moment, which can result in less ideal load sharing compared to medial plating, especially with conventional compression plates. However, modern locking plate technology has mitigated some of these concerns by providing angular stable constructs that function as internal fixators, independent of plate-to-bone compression.
- Advantage : The major benefit is the superior soft tissue coverage provided by the anterior compartment muscles. This significantly reduces the risk of wound complications, hardware prominence, and secondary infections, particularly in compromised soft tissue envelopes. The muscular envelope acts as a biological buffer, enhancing vascularity and promoting healing.
- Disadvantage : Requires careful retraction of the anterior compartment musculature, potentially increasing the risk of injury to the deep fibular nerve and anterior tibial vessels, especially in inexperienced hands. The contour of the lateral tibia can also be more complex to match with a plate.
The decision to plate medially or anterolaterally often hinges on fracture morphology, soft tissue quality, surgeon preference, and specific implant design. Minimally Invasive Plate Osteosynthesis (MIPO) techniques have further refined the approach, allowing for plate insertion through smaller incisions while preserving periosteal blood supply.
Indications & Contraindications
The anterior approach to the tibia is a cornerstone in the surgical management of various traumatic, degenerative, and neoplastic conditions affecting the tibial shaft. Its versatility, direct access, and robust exposure make it suitable for a wide array of indications, while specific contraindications guide the surgeon towards alternative strategies to optimize patient outcomes.
Indications
The anterior approach offers safe, easy access to the medial (subcutaneous) and lateral (extensor) surfaces of the tibia. It is used for the following:
-
Open Reduction and Internal Fixation (ORIF) of Tibial Fractures :
- Complex Tibial Shaft Fractures : Especially comminuted, segmental, spiral, or oblique fractures not amenable to intramedullary nailing (e.g., very proximal or distal fractures extending into the metaphysis/epiphysis, or fractures with significant metaphyseal involvement where nailing cannot achieve adequate stability).
- Open Fractures : Facilitates thorough debridement and stable fixation, particularly Gustilo-Anderson Type II and III open fractures where direct visualization is essential for managing soft tissue and bone fragments.
- Floating Knee Injuries : Part of the management strategy for combined ipsilateral femoral and tibial fractures.
- Adjunctive Fixation : In conjunction with intramedullary nailing for highly comminuted diaphyseal-metaphyseal fractures where additional plate fixation (e.g., "nail-plate" construct) is required to restore length, alignment, or provide rotational control.
- Periprosthetic Fractures : Around knee or ankle prostheses where nailing is not feasible.
-
Bone Grafting for Delayed Union or Nonunion of Fractures :
- Provides direct access for decortication, debridement of fibrous tissue at the nonunion site, and application of autogenous or allogenous bone graft material.
- Often combined with revision fixation to provide a stable biomechanical environment.
-
Excision of Sequestra or Saucerization in Patients with Osteomyelitis :
- Critical for debridement of infected and necrotic bone (sequestrum) and creation of a healthy vascularized bed (saucerization) in chronic osteomyelitis. The direct approach allows for meticulous removal of all devitalized tissue.
-
Excision and Biopsy of Tumors :
- Primary or metastatic bone tumors of the tibial shaft. The approach permits adequate exposure for en-bloc resection or incisional biopsy, crucial for accurate staging and definitive oncologic management.
-
Osteotomy :
- Corrective osteotomies for malunions, angular deformities (e.g., genu varum, genu valgum), or limb length discrepancies. This approach allows for precise bone cuts and stable internal fixation.
-
Hardware Removal :
- Access for removal of previously implanted plates, screws, or other hardware, especially in cases of infection, hardware prominence, or planned revision.
-
Acute Compartment Syndrome :
- Though typically addressed via specific fasciotomy incisions, direct anterior approach during fracture fixation may be extended to perform concurrent anterior and lateral compartment fasciotomies if clinical suspicion for compartment syndrome arises intraoperatively or preoperatively.
Plates applied to the subcutaneous surface of the tibia are placed correctly biomechanically on the medial (tensile) side of the bone; they also are easier to contour there. Some surgeons prefer to use the lateral surface for plating, however, to avoid the problems of subcutaneous placement which may result in breakdown of the wound.
Contraindications
The anterior approach is the preferred approach to the tibia except when the skin is scarred or has draining sinuses in it. Other significant contraindications include:
- Severe Soft Tissue Compromise : Extensive skin loss, severe degloving injuries, presence of active infection with significant purulence, or multiple draining sinuses over the planned incision site. In such cases, alternative approaches (e.g., posteromedial, posterolateral) or staged procedures with soft tissue reconstruction may be necessary.
- Vascular Impairment : Pre-existing severe peripheral vascular disease or local vascular compromise that could be exacerbated by extensive dissection or retraction, especially regarding the anterior tibial artery.
-
Fractures best managed by other approaches
:
- Isolated fibular fractures.
- Proximal or distal tibial fractures with primary involvement of articular surfaces, where dedicated intra-articular approaches (e.g., anteromedial, anterolateral for tibial plateau; combined approach for pilon fractures) offer superior visualization.
- Most isolated, stable tibial shaft fractures, where intramedullary nailing is typically the preferred treatment due to biological advantages and lower complication rates, unless specific contraindications to nailing exist.
- Prior Surgery with Extensive Scarring : May increase dissection difficulty, risk of neurovascular injury, and wound complications.
- Patient Factors : Severe comorbidities that preclude prolonged surgery or general anesthesia.
Table: Operative vs. Non-Operative Indications for Tibial Fractures
| Indication Type | Operative Treatment (Anterior Approach often applicable) | Non-Operative Treatment (Rare for shaft fractures requiring fixation) |
|---|---|---|
| Fractures | - Displaced, unstable tibial shaft fractures | - Minimally displaced, stable hairline fractures |
| - Open tibial fractures (Gustilo Type I-IIIA) | - Select non-displaced stress fractures | |
| - Segmental or highly comminuted fractures | - Rarely, very stable, non-displaced spiral/oblique patterns | |
| - Fractures with associated neurovascular injury | ||
| - Fractures with compartment syndrome | ||
| - Failed non-operative treatment (e.g., loss of reduction) | ||
| Nonunion/Malunion | - Symptomatic nonunion or delayed union requiring revision | - Asymptomatic nonunion (rarely) |
| - Significant malunion causing functional impairment | - Minor malunion with no functional deficit | |
| Infection | - Chronic osteomyelitis with sequestrum/abscess | - Cellulitis without bone involvement (managed with antibiotics) |
| - Infected nonunion | ||
| Tumors | - Biopsy or excision of bone tumors | - Benign, asymptomatic lesions amenable to observation |
| - Curettage and bone grafting for benign lesions | ||
| Deformity | - Corrective osteotomy for angular/rotational deformity | - Congenital deformities managed conservatively in infancy |
| Hardware Related | - Symptomatic hardware prominence/infection | - Asymptomatic hardware (patient preference for retention) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical determinants of surgical success and patient safety when utilizing the anterior approach to the tibia.
Pre-Operative Planning
- Patient Assessment : A thorough history and physical examination are mandatory. This includes evaluating the neurovascular status of the limb, assessing the soft tissue envelope for skin integrity, prior incisions, scars, or active infection. Assess for comorbidities that may affect wound healing or anesthesia.
-
Imaging Review
:
- Plain Radiographs : Standard anteroposterior, lateral, and oblique views of the entire tibia, including knee and ankle joints, are essential. These help characterize fracture pattern, displacement, comminution, and bone quality. For nonunions, views should include stress radiographs if instability is suspected.
- Computed Tomography (CT) Scan : Indicated for complex fracture patterns (especially articular extension), malunions, or tumors. CT provides detailed 3D information on fracture morphology, bone loss, and helps delineate tumor margins.
- Magnetic Resonance Imaging (MRI) : Useful for assessing soft tissue injuries, suspected osteomyelitis (marrow edema, sequestra, sinus tracts), and tumor characterization.
- Angiography/Doppler Ultrasound : If significant vascular injury is suspected, particularly in high-energy trauma or open fractures.
-
Surgical Strategy Formulation
:
- Approach Selection : Confirm the anterior approach is optimal based on pathology and soft tissue status. Determine whether medial or anterolateral plating is preferred.
- Implant Selection : Choose appropriate fixation hardware (e.g., dynamic compression plate, locking compression plate, specific length and screw types). Consider the need for bone grafting material (autograft, allograft, bone graft substitutes). Plan screw trajectories to maximize purchase and avoid neurovascular structures.
- Tourniquet Decision : Assess the necessity and potential risks of tourniquet use.
- Contingency Planning : Prepare for potential intraoperative challenges, such as unexpected comminution, difficult reduction, or soft tissue deficiencies. Have alternative implants or techniques readily available.
- Antibiotic Prophylaxis : Administer broad-spectrum intravenous antibiotics pre-incision, particularly for open fractures or procedures involving hardware implantation.
Patient Positioning
The anterior approach mandates specific patient positioning to provide optimal exposure, facilitate limb manipulation, and ensure safe tourniquet application if used.
-
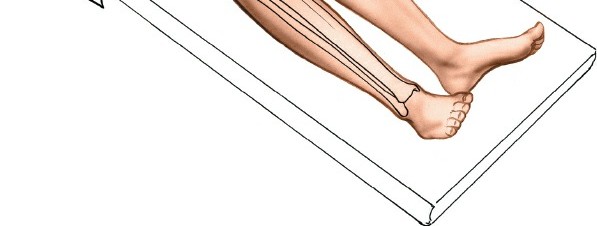
Supine Position
: The patient is placed supine on a radiolucent operating table.
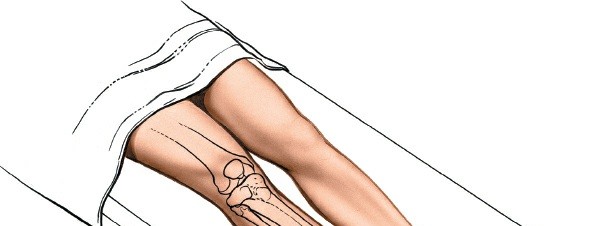
- Limb Support : The entire lower extremity from hip to foot should be prepped and draped to allow for full range of motion and unimpeded C-arm access. A bump can be placed under the ipsilateral hip to internally rotate the leg slightly, bringing the anterior aspect into a more favorable position.
- Tourniquet Application : The use of a tourniquet is optional. Tourniquets should not be used if this approach is to be used in conjunction with the exploration of an open wound, as it can mask active bleeding and prevent adequate debridement. If you wish to use a tourniquet, exsanguinate the limb by elevating it for 3 to 5 minutes, then inflate a tourniquet. A pneumatic tourniquet is typically applied high on the thigh. Ensure proper padding to prevent skin damage or nerve compression. The tourniquet pressure should be appropriate for the patient's systolic blood pressure (e.g., 100 mmHg above systolic for normotensive patients, generally not exceeding 300-350 mmHg). Monitor tourniquet time closely, typically limiting inflation to 90-120 minutes.
- C-arm Access : Ensure the C-arm can be positioned to obtain high-quality anteroposterior and lateral images of the entire operative field without contamination of the sterile field. This often requires placing the C-arm perpendicular to the table or utilizing a mobile table that allows for easy repositioning.
Detailed Surgical Approach / Technique
The anterior approach to the tibia requires precise dissection, careful identification of anatomical structures, and meticulous execution of reduction and fixation techniques. The following steps outline a comprehensive surgical protocol.
1. Incision
The skin incision is crucial for providing adequate exposure while minimizing soft tissue damage and optimizing wound healing.
*
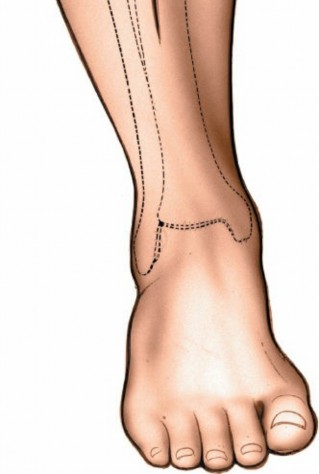
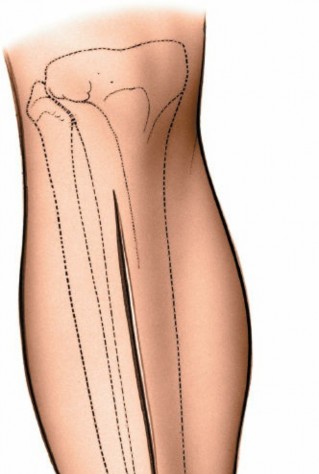
Location
: A longitudinal incision is made over the anteromedial aspect of the tibia. The exact placement depends on the specific pathology. For diaphyseal fractures, the incision should be centered over the fracture site, extending proximally and distally to allow for adequate plate length and screw placement.
*
Length
: The incision should be long enough to allow visualization of at least two screw holes proximal and two distal to the fracture, ensuring sufficient working space for reduction and plate application. For MIPO techniques, multiple smaller incisions are used.
*
Skin Only
: The incision is made through the skin and subcutaneous tissue down to the deep fascia.
Incision over the anterior aspect of the tibia, ensuring adequate length for exposure.
2. Superficial Dissection
After incising the skin, the subcutaneous fat is encountered.
*
Medial Side Protection
: Along the medial aspect of the incision, carefully identify and protect the
saphenous vein
and
saphenous nerve
. These structures run subcutaneously and are susceptible to injury during incision or retraction. Gentle blunt dissection parallel to their course can help minimize damage.
*
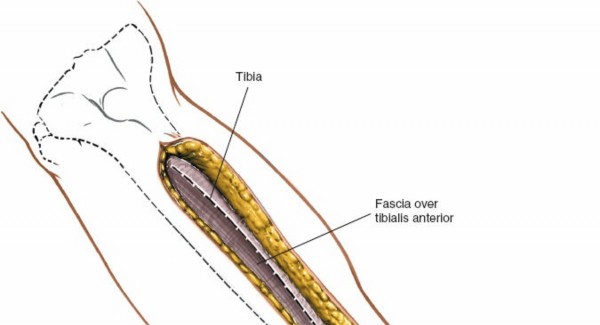
Deep Fascia (Crural Fascia)
: Continue dissection through the subcutaneous tissue to expose the deep crural fascia, which invests the muscles of the lower leg.

Superficial dissection revealing the deep crural fascia and careful retraction of subcutaneous tissues.
3. Internervous Plane & Muscle Dissection
The anterior approach can expose either the medial subcutaneous surface or the anterolateral surface of the tibia, dictated by the chosen plating strategy.
A. Medial (Subcutaneous) Approach
- Direct Periosteal Incision : This is the most direct route. Once the deep fascia is exposed, a longitudinal incision is made through the fascia and periosteum directly over the desired portion of the medial tibial shaft.
- Subperiosteal Elevation : Using a sharp periosteal elevator (e.g., Cobb, Freer), the periosteum is carefully elevated from the medial surface of the tibia. It is critical to preserve as much periosteal attachment as possible, especially in comminuted fractures, to maintain bone vascularity and promote healing. Avoid extensive stripping.
B. Anterolateral Approach
This approach utilizes the interval between the tibialis anterior muscle and the extensor digitorum longus (EDL)/extensor hallucis longus (EHL) muscles.
*
Fascial Incision
: Incise the deep crural fascia longitudinally, typically slightly lateral to the anterior border of the tibia.
*
Muscle Retraction
:
*
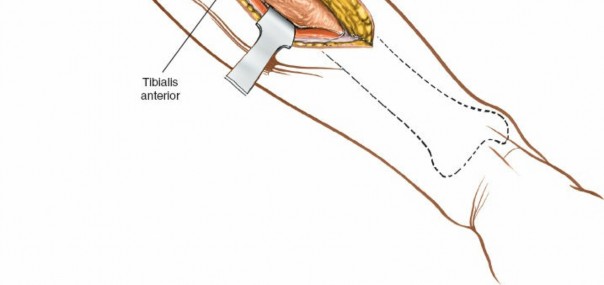
Tibialis Anterior
: This muscle is identified and carefully retracted medially. Its origin is from the lateral condyle and proximal lateral shaft of the tibia, and the interosseous membrane.
*
Extensor Digitorum Longus (EDL) and Extensor Hallucis Longus (EHL)
: These muscles are identified and retracted laterally. The EHL lies deep to the tibialis anterior and EDL in the mid-leg.
*
Neurovascular Bundle Protection
: The
anterior tibial artery and veins
and the
deep fibular nerve
lie on the interosseous membrane, between the tibialis anterior and the EHL/EDL. These structures must be identified and carefully protected throughout the entire dissection. Avoid aggressive retraction that could stretch or compress the nerve or vessels. Dissection typically proceeds just lateral to the anterior border of the tibia, exposing the lateral surface of the bone.

Identification and careful retraction of the tibialis anterior muscle medially, exposing deeper structures and internervous planes.
Cross-sectional anatomy illustrating the compartmentalization of the leg and the position of neurovascular structures relative to the tibia and muscle groups.
4. Periosteal Incision & Exposure
Once the desired surface of the tibia (medial or anterolateral) is reached, a longitudinal incision is made through the periosteum.
*
Subperiosteal Dissection
: Using a periosteal elevator, the periosteum is gently elevated from the bone surface to create a working space for plate application. Limit subperiosteal stripping to the minimum necessary for plate placement to preserve blood supply. In cases of significant comminution or open fractures, a less aggressive periosteal elevation (indirect reduction) is often preferred to promote biological healing.
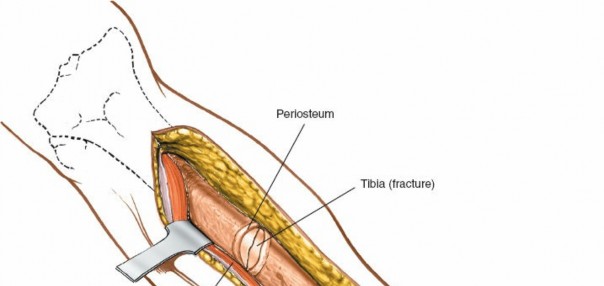
Exposure of the tibial shaft following periosteal incision and elevation, preparing the bone for reduction and fixation.
5. Fracture Reduction
Achieving anatomical reduction is paramount for optimal biomechanics and healing.
*
Indirect Reduction Techniques (for comminuted fractures)
: Utilize external traction, distraction devices, or plate as a template to restore length, alignment, and rotation without directly manipulating fracture fragments.
*
Direct Reduction Techniques (for simple fracture patterns)
:
*
Traction and Counter-traction
: Applied to the limb to restore length.
*
Manipulation
: Using bone hooks, large reduction clamps (e.g., Verbrugge, pointed reduction clamp), or elevator to align fragments.
*
Provisional Fixation
: K-wires or small external fixator clamps can be used to hold reduction temporarily.
*
Fluoroscopic Guidance
: Essential to confirm anatomical alignment in multiple planes, especially for rotational control.
6. Internal Fixation (Plating)
The choice of plate and its application technique depends on the fracture pattern, bone quality, and desired stability.
-
Plate Contour and Placement
:
- Medial Plating : Apply the plate directly to the subcutaneous medial surface. Contour carefully to match the tibial anatomy and minimize prominence. This is often the tensile side, ideal for compression plating.
- Anterolateral Plating : Requires careful retraction of anterior compartment muscles. The plate is applied to the lateral aspect of the tibia. While offering better soft tissue coverage, it's considered the compression side, potentially less biomechanically favorable for conventional compression, but highly effective with locking plates.
-
Screw Application
:
- Lag Screws : For oblique or spiral fractures, lag screws across the fracture plane can provide interfragmentary compression, achieving absolute stability.
- Compression Screws : Dynamic compression plates (DCP) or limited contact dynamic compression plates (LC-DCP) can achieve axial compression.
- Locking Screws : Locking Compression Plates (LCP) utilize locking screws that provide angular stability, converting the plate into an internal fixator. This is particularly useful in osteoporotic bone, comminuted fractures (bridge plating), or when preserving periosteal blood supply is critical.
-
Minimally Invasive Plate Osteosynthesis (MIPO)
:
- This technique involves inserting a plate through small proximal and distal incisions, using instruments (e.g., plate loaders, percutaneous guides) to tunnel the plate submuscularly or subfascially along the bone.
-
Indirect reduction techniques are paramount to preserve soft tissue attachments and blood supply. Percutaneous screw insertion is guided by fluoroscopy. MIPO is particularly valuable for bridge plating comminuted fractures, minimizing soft tissue disruption.
Intraoperative view demonstrating fracture reduction with reduction clamps and provisional wire fixation, prior to definitive plate application.
Final internal fixation with a locking plate and screws, ensuring stable construct and adequate purchase both proximally and distally.
7. Wound Closure
Meticulous wound closure is essential to minimize complications.
*
Irrigation
: Thoroughly irrigate the wound with sterile saline to remove debris and reduce bacterial load.
*
Hemostasis
: Achieve complete hemostasis.
*
Periosteum/Fascia
: Close the periosteum (if significantly incised and not excessively stripped) and deep fascia with absorbable sutures, if possible, to aid in muscle containment and prevent hernia.
*
Subcutaneous Tissue
: Close the subcutaneous layers with absorbable sutures to obliterate dead space and reduce tension on the skin.
*
Skin
: Close the skin with non-absorbable sutures or staples. Avoid excessive tension.
*
Drain
: A suction drain may be considered, especially in cases of extensive debridement or patients with high bleeding risk, but its routine use is debated and not universally recommended for clean cases.
Complications & Management
Despite meticulous surgical technique, the anterior approach to the tibia is not without potential complications. Understanding these risks, their incidence, and effective management strategies is crucial for optimizing patient outcomes.
Common Complications
-
Wound Complications
:
- Incidence : High, particularly with medial plating due to subcutaneous location. Reported rates range from 5-30%. Factors include severe soft tissue injury (open fractures), medial approach, diabetes, smoking, and extensive periosteal stripping.
- Manifestations : Superficial infection, deep infection, wound dehiscence, skin necrosis, hematoma formation.
-
Infection
:
- Incidence : Deep infection, including osteomyelitis, is a devastating complication. Rates vary significantly depending on fracture type (open vs. closed), ranging from 1-5% for closed fractures to over 30% for severe open fractures.
- Risk Factors : High-energy trauma, open fractures, prolonged surgery, poor soft tissue coverage, medical comorbidities.
-
Nonunion/Delayed Union
:
- Incidence : Tibial shaft fractures have a higher nonunion rate than many other long bones, ranging from 10-20% for closed fractures and up to 50% for open or highly comminuted fractures.
- Causes : Inadequate reduction or fixation stability, extensive soft tissue damage, poor vascularity, infection, smoking, NSAID use.
-
Malunion
:
- Incidence : Variable, depending on the definition (e.g., >5-10 degrees angulation, >1 cm shortening, rotational malalignment). Can range from 5-15%.
- Causes : Inadequate intraoperative assessment of alignment, rotational errors, loss of reduction post-operatively.
-
Neurovascular Injury
:
- Incidence : Rare but serious. Deep fibular nerve (motor/sensory deficit in anterior compartment) and anterior tibial artery/veins (ischemia, compartment syndrome) are most at risk during anterolateral dissection. Saphenous nerve (sensory deficit along medial leg/ankle) is vulnerable during medial dissection.
- Causes : Direct trauma from instruments, excessive or prolonged retraction, thermal injury from drilling.
-
Compartment Syndrome
:
- Incidence : Approximately 1-10% of tibial shaft fractures, higher in high-energy trauma. Can be missed if not vigilant.
- Causes : Increased intracompartmental pressure due to hemorrhage, edema, or reperfusion injury, compromising neurovascular supply to muscles.
-
Hardware Prominence/Irritation
:
- Incidence : Common, particularly with medial plating due to thin soft tissue cover.
- Manifestations : Pain, discomfort, localized skin irritation, bursitis over hardware. May necessitate elective hardware removal.
-
Refracture After Hardware Removal
:
- Incidence : 2-5%.
- Causes : Premature hardware removal before adequate cortical remodeling, presence of stress risers (e.g., empty screw holes), or persistent bone weakness.
-
Chronic Regional Pain Syndrome (CRPS)
:
- Incidence : Variable, 1-5%.
- Causes : Complex multifactorial neuropathic pain syndrome.
Management & Salvage Strategies
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Wound Dehiscence/Necrosis | 5-30% | - Local wound care, debridement of necrotic tissue. |
| - Vacuum-assisted closure (VAC) therapy. | ||
| - Soft tissue coverage procedures: local rotational flaps, gastrocnemius flap, soleus flap, free flap reconstruction (e.g., free fibula, latissimus dorsi, anterolateral thigh flap) in severe cases. | ||
| Infection (Deep/Osteomyelitis) | 1-30% | - Aggressive surgical debridement of all infected and necrotic tissue (bone, soft tissue). |
| - Culture-guided antibiotic therapy (long-term, IV followed by oral). | ||
| - Hardware retention (if stable and necessary) or removal/exchange (if unstable or infected). | ||
| - Debridement with dead space management (antibiotic beads, cement spacers). | ||
| - Soft tissue coverage (as above) if necessary. | ||
| - For infected nonunion: staged treatment with external fixation, debridement, antibiotics, followed by definitive internal fixation and bone grafting after infection control. | ||
| Nonunion/Delayed Union | 10-50% | - Revision surgery: Re-open, debride nonunion site, refresh bone ends. |
| - Bone grafting: Autogenous cancellous bone graft (iliac crest), allograft, bone morphogenetic proteins (BMPs), synthetic bone grafts. | ||
| - Enhance stability: Exchange intramedullary nailing, revision plating with larger/stronger construct, dynamic compression or locking plates. | ||
| - Biological augmentation: Pulsed electromagnetic fields (PEMF), low-intensity pulsed ultrasound (LIPUS). | ||
| Malunion | 5-15% | - Corrective osteotomy (wedge osteotomy, dome osteotomy) to restore anatomical alignment, length, and rotation. |
| - Internal fixation with plates/screws or external fixation to maintain correction. | ||
| Neurovascular Injury | <1% | - Nerve Injury : Observation for neurapraxia. Neurolysis or nerve repair (grafting) for transection. Tendon transfers for persistent functional deficit. |
| - Vascular Injury : Surgical exploration, repair (primary repair, vein graft), or bypass. Urgent revascularization is critical for limb salvage. | ||
| Acute Compartment Syndrome | 1-10% | - Immediate four-compartment fasciotomy of the lower leg (longitudinal incisions). |
| - Leaving skin open, delayed primary closure or split-thickness skin graft after swelling subsides (2-5 days). | ||
| Hardware Prominence/Irritation | Common | - Elective hardware removal after fracture union, typically 12-18 months post-surgery. |
| Refracture After Hardware Removal | 2-5% | - Delayed hardware removal until radiographic evidence of cortical remodeling. |
| - Patient education on activity restrictions post-removal, especially for high-impact activities. Consider prophylactic plating in high-risk patients if hardware removal is essential. | ||
| Chronic Regional Pain Syndrome (CRPS) | 1-5% | - Multidisciplinary pain management: physical therapy, occupational therapy, neuropathic pain medications (e.g., gabapentin, pregabalin), regional nerve blocks, spinal cord stimulation. Early recognition and treatment are key. |
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is integral to achieving optimal functional outcomes following anterior approach tibial surgery. Rehabilitation aims to restore strength, range of motion, proprioception, and functional independence while protecting the surgical repair. The specific timeline and weight-bearing progression are highly individualized, depending on the fracture pattern, stability of fixation, bone quality, soft tissue integrity, and patient's general health.
Phase 1: Immediate Post-Operative (Weeks 0-2)
- Goals : Pain and swelling control, wound healing, protection of fixation, initiation of gentle range of motion (ROM).
- Weight-Bearing (WB) : Typically non-weight bearing (NWB) to touch-down weight bearing (TDWB) on the operative limb. For very stable constructs, partial weight bearing (PWB) may be initiated earlier.
-
Interventions
:
- Pain Management : Scheduled analgesics, nerve blocks, multimodal approach.
- Wound Care : Daily dressing changes, monitoring for signs of infection or dehiscence.
- Elevation : Consistent elevation of the limb (above heart level) to minimize swelling.
- Cryotherapy : Application of ice packs to reduce pain and edema.
- Gentle ROM : Active and passive ankle ROM exercises (dorsiflexion, plantarflexion, inversion, eversion) within pain-free limits. Gentle knee flexion/extension exercises as tolerated.
- Muscle Activation : Isometric quadriceps and gluteal sets to prevent atrophy.
- Assistive Devices : Training with crutches or a walker for NWB/TDWB ambulation.
Phase 2: Early Mobilization & Progressive Weight-Bearing (Weeks 2-6)
- Goals : Gradual increase in weight-bearing, restoration of full pain-free ROM, initiation of gentle strengthening.
- Weight-Bearing : Progression from TDWB to partial weight bearing (PWB) as tolerated, guided by clinical and radiographic signs of healing. This typically involves 25-50% body weight.
-
Interventions
:
- Continued ROM : Progress ankle and knee ROM exercises. Incorporate gentle stretching.
-
Strengthening
:
- Isometric strengthening of anterior compartment muscles (e.g., tibialis anterior isometrics).
- Initiate active-assisted and then active exercises for ankle and knee.
- Gluteal and core strengthening.
- Gait Training : Emphasis on proper gait mechanics, minimizing compensatory patterns, and progressively increasing load through the operative limb.
- Edema Management : Compression stockings or wraps if swelling persists.
- Scar Mobilization : Gentle massage once the wound is completely healed to prevent adhesions.
Phase 3: Intermediate Strengthening & Proprioception (Weeks 6-12)
- Goals : Achieve full weight-bearing, enhance muscle strength and endurance, improve balance and proprioception.
- Weight-Bearing : Progress to full weight bearing (FWB) as tolerated, contingent on radiographic evidence of early callus formation and clinical stability.
-
Interventions
:
-
Advanced Strengthening
:
- Progressive resistive exercises (PRE) for all lower extremity muscle groups using resistance bands, light weights, or gym equipment.
- Concentrated strengthening of calf muscles, quadriceps, and hamstrings.
- Closed kinetic chain exercises (e.g., mini-squats, lunges, calf raises).
- Proprioceptive Training : Balance exercises on stable surfaces, then unstable surfaces (e.g., foam pad, wobble board). Single-leg stance activities.
- Cardiovascular Fitness : Stationary cycling, elliptical trainer, swimming (once wounds are fully closed) to maintain overall fitness.
- Gait Refinement : Focus on normalizing stride length, cadence, and symmetry.
-
Advanced Strengthening
:
Phase 4: Advanced Functional Training & Return to Activity (Months 3-6+)
- Goals : Achieve maximum strength, power, agility, and return to pre-injury activity levels, including sport-specific demands.
- Weight-Bearing : Full, unrestricted weight-bearing.
-
Interventions
:
- High-Level Strengthening : Plyometric exercises (jumping, hopping), agility drills (cutting, pivoting), sport-specific functional exercises.
- Endurance Training : Running, hiking, escalating cardiovascular intensity.
- Impact Loading : Gradual introduction of impact activities, starting with low-impact and progressing to high-impact sports.
- Biomechanical Analysis : Assessment of movement patterns to identify and correct any residual deficits.
- Patient Education : Guidance on long-term activity modification, importance of proper footwear, and recognizing signs of overuse or impending complications. Hardware removal may be considered after 12-18 months if symptomatic or biomechanically necessary, followed by a short period of restricted activity.
A multidisciplinary approach involving the orthopedic surgeon, physical therapist, and occupational therapist is essential to tailor rehabilitation to individual patient needs and ensure a safe and effective return to function.
Summary of Key Literature / Guidelines
The anterior approach to the tibia has a long-standing history in orthopedic surgery, with an evolving body of literature guiding its applications and techniques. Key insights from current research and clinical guidelines provide evidence-based principles for its safe and effective use.
-
Plating Strategies (Medial vs. Anterolateral) :
- Soft Tissue Considerations : Contemporary literature consistently highlights the improved soft tissue envelope and reduced wound complications associated with anterolateral plating compared to the medial subcutaneous approach. Studies by various authors underscore the biomechanical trade-offs but often favor the anterolateral approach for its biological advantages in minimizing skin necrosis and hardware prominence, especially in patients with compromised soft tissues or those requiring delayed closure.
- Biomechanics : While the medial tibia is the tension side, ideal for traditional compression plating, modern locking plates (LCPs) provide fixed-angle constructs. This allows for biomechanically sound fixation on either the medial or anterolateral surface, as the plate acts as an internal fixator independent of plate-to-bone compression. The choice often leans on soft tissue factors and surgeon familiarity rather than absolute biomechanical superiority of one surface with LCPs.
-
Minimally Invasive Plate Osteosynthesis (MIPO) :
- Benefits : MIPO techniques for tibial shaft fractures fixed via the anterior approach have gained significant traction. Numerous studies demonstrate reduced periosteal stripping, preserved vascularity, lower rates of infection, and potentially faster union times compared to traditional open techniques. This is particularly relevant for comminuted or open fractures where biological preservation is paramount.
- Challenges : MIPO requires significant fluoroscopic expertise to ensure accurate plate positioning, reduction, and percutaneous screw insertion, mitigating risks of malunion or neurovascular injury.
-
Indications for Plating vs. Intramedullary Nailing :
-
Tibial Shaft Fractures
: Intramedullary nailing remains the gold standard for most diaphyseal tibial fractures due to its load-sharing capabilities, high union rates, and lower soft tissue morbidity. However, plating via the anterior approach is preferred for specific scenarios:
- Proximal and Distal Metaphyseal/Articular Extension : Where intramedullary nails may not provide adequate stability or interfere with joint reconstruction.
- Highly Comminuted or Segmental Fractures : Especially in conjunction with nailing (nail-plate constructs) or as the primary fixation method when nailing is not feasible.
- Open Fractures with Significant Soft Tissue Loss : Where direct visualization and thorough debridement are critical, and plating provides stable fixation for subsequent soft tissue reconstruction.
- Malunions/Nonunions : For corrective osteotomies, debridement, and bone grafting, where precise anatomical restoration is required.
- Nonunion Rates : Nonunion rates for tibial shaft fractures treated with plating can be higher than with nailing, particularly for open and comminuted fractures, underscoring the importance of biological considerations and adjunctive bone grafting when using plates.
-
Tibial Shaft Fractures
: Intramedullary nailing remains the gold standard for most diaphyseal tibial fractures due to its load-sharing capabilities, high union rates, and lower soft tissue morbidity. However, plating via the anterior approach is preferred for specific scenarios:
-
Management of Open Tibial Fractures :
- Guideline Adherence : The anterior approach is frequently used for open tibial fractures. Guidelines emphasize urgent debridement, copious irrigation, broad-spectrum antibiotics, and stable fixation. The role of staged debridement and early soft tissue coverage by plastic surgery is critical to minimize infection rates and optimize healing.
-
Complication Rates and Mitigation :
- Wound Complications : Remain a primary concern, especially for medial plating. Strategies to mitigate include meticulous soft tissue handling, appropriate incision placement, avoiding excessive periosteal stripping, tension-free wound closure, and considering anterolateral plating or MIPO techniques.
- Infection : Adherence to sterile technique, appropriate antibiotic prophylaxis, thorough debridement, and early soft tissue coverage are cornerstones of prevention.
- Neurovascular Injury : Knowledge of anatomy, careful dissection, and gentle retraction are crucial. Intraoperative monitoring (e.g., nerve stimulator) can be considered in high-risk cases.
In summary, the anterior approach to the tibia is a vital surgical technique, particularly for complex scenarios where direct visualization, robust fixation, and meticulous soft tissue management are required. Evolving evidence supports the judicious use of locking plates and MIPO techniques, often favoring anterolateral placement, to optimize outcomes and minimize complications in this challenging anatomical region. Continued adherence to sound surgical principles and evidence-based guidelines is paramount.
Clinical & Radiographic Imaging