Introduction to Elbow Contracture and Stiffness
The elbow joint is highly susceptible to post-traumatic stiffness due to its highly congruent osseous anatomy, complex capsuloligamentous structures, and profound propensity for robust fibroblastic responses following injury. A normal elbow possesses a range of motion (ROM) from 0 degrees of extension to 140 degrees of flexion, with 70 to 80 degrees of both pronation and supination. However, the functional arc of motion—as classically described by Morrey—requires only 30 to 130 degrees of flexion and 50 degrees of pronation and supination to perform most activities of daily living (ADLs).
When conservative measures, including aggressive physical therapy and dynamic or static-progressive splinting, fail to restore this functional arc after 6 months, operative intervention is indicated. The surgical release of an elbow contracture demands a comprehensive understanding of elbow biomechanics, precise soft-tissue handling, and a strategic approach to both the anterior and posterior compartments.
Clinical Pearl: The anterior capsule is the primary soft-tissue restraint to elbow extension, while the posterior capsule restricts flexion. A comprehensive release almost universally requires addressing both compartments, regardless of whether the primary clinical deficit is in flexion or extension.
Preoperative Evaluation and Biomechanical Considerations
A meticulous preoperative assessment is paramount. The surgeon must differentiate between intrinsic causes of stiffness (e.g., intra-articular adhesions, osteochondral defects, malunited articular fractures) and extrinsic causes (e.g., capsular contracture, collateral ligament scarring, heterotopic ossification, extra-articular malunions).
Standard anteroposterior and lateral radiographs are mandatory to assess joint congruency and identify osteophytes or heterotopic ossification (HO). A computed tomography (CT) scan with 3D reconstruction is highly recommended to precisely map the location of ectopic bone, evaluate the olecranon and coronoid fossae for osseous impingement, and plan the extent of bony debridement.
Anterior and Posterior Release of Elbow Contracture (Morrey Technique)
The extensile lateral approach, popularized by Morrey, is a workhorse technique for addressing severe elbow contractures. It allows simultaneous access to the anterior and posterior compartments while preserving the critical medial structures, provided the dissection respects the anatomic boundaries.
Patient Positioning and Preparation
- Place the patient in the supine position on the operating table.
- Position a sandbag or a rolled towel under the ipsilateral scapula to elevate the shoulder and allow the arm to rest comfortably across the chest.
- Apply a sterile tourniquet high on the brachium to ensure a bloodless surgical field.
- Drape the extremity free, allowing full, unencumbered manipulation of the elbow through its maximum arc of motion. Bring the forearm across the abdomen to expose the lateral aspect of the elbow.
The Extensile Lateral (Kocher) Approach
The surgical exposure begins with an extensile modification of the classic Kocher approach, designed to provide panoramic access to the lateral column of the distal humerus and the radiocapitellar joint.
- Make an extensive longitudinal skin incision (approximately 15 cm in length). Begin proximally along the lateral supracondylar ridge of the humerus.
- Continue the incision distally, passing directly over the lateral epicondyle, and terminate it over the subcutaneous border of the proximal ulna.
- Proximally, carry the dissection sharply down to the lateral supracondylar ridge. Identify the interval between the triceps posteriorly and the brachioradialis anteriorly.
- Distally, incise the deep fascia along the lateral margin of the triceps and develop the internervous plane between the anconeus (radial nerve) and the extensor carpi ulnaris (posterior interosseous nerve).
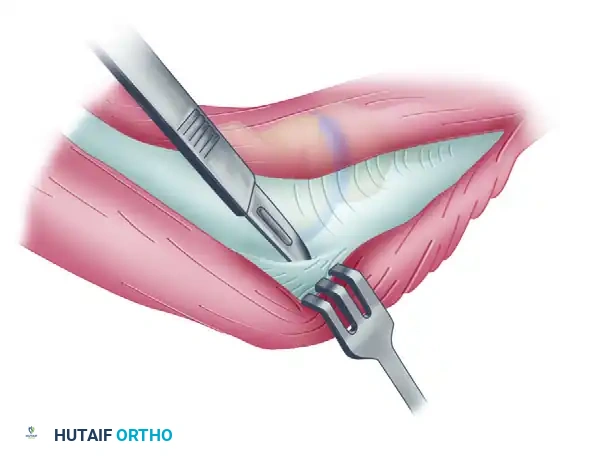
Deep Dissection and Anterior Capsulectomy
The goal of the anterior dissection is to safely separate the neurovascular structures from the anterior capsule before performing the capsulectomy.
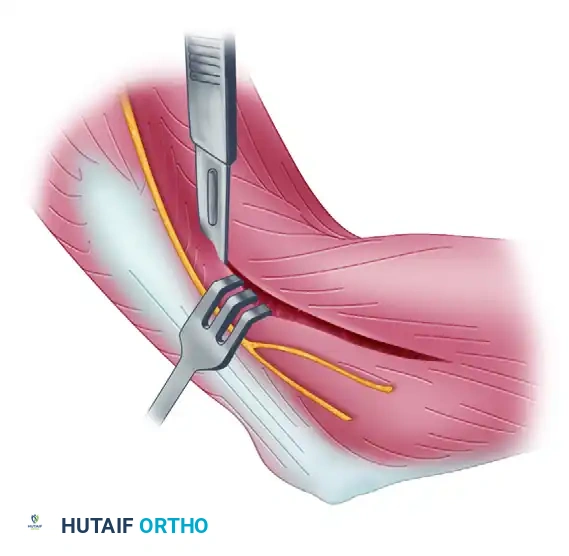
- Carefully elevate the brachialis muscle belly off the anterior joint capsule. This must be done meticulously, as the brachialis serves as a protective barrier for the brachial artery and the median nerve.
- Place blunt retractors (such as right-angle or Hohmann retractors) deep to the brachioradialis and brachialis muscles. This maneuver safely retracts the anterior neurovascular bundle and exposes the underlying, thickened anterior joint capsule.
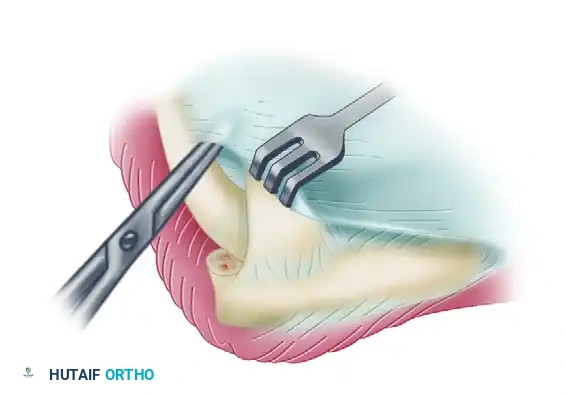
- Perform a comprehensive anterior capsulectomy, proceeding systematically from lateral to medial.
- Critical Step: Identify and preserve the lateral collateral ligament (LCL) complex, specifically the lateral ulnar collateral ligament (LUCL). The capsulectomy must stay strictly anterior to the LCL origin on the lateral epicondyle to prevent iatrogenic posterolateral rotatory instability (PLRI).
Surgical Warning: When extending the anterior capsulectomy medially, maintain the dissection strictly within the capsular plane. Straying anteriorly risks injury to the median nerve and brachial artery, while straying too far medially and posteriorly risks injury to the ulnar nerve.
Posterior Dissection and Capsulectomy
Once the anterior release is complete, attention is turned to the posterior compartment to restore elbow flexion.
- To preserve periosteal continuity and optimize triceps function postoperatively, elevate the triceps tendon subperiosteally from the posterior aspect of the humerus and the tip of the olecranon.
- Retract the mobilized triceps posteriorly and medially to expose the underlying posterior joint capsule and the olecranon fossa.
- Perform a posterior capsulectomy, again proceeding from lateral to medial.
- Ulnar Nerve Precaution: Take extreme care not to venture too far medially during the posterior capsulectomy. The ulnar nerve lies immediately posterior to the medial epicondyle in the cubital tunnel. If extensive medial capsular release or medial osteophyte excision is required, a separate medial incision to decompress and protect the ulnar nerve is strongly advised.
Bony Debridement and Impingement Clearance
Soft-tissue release alone is often insufficient if osseous impingement exists. The surgeon must dynamically test the elbow and address any bony blocks.
- Completely extend the elbow. If extension remains incomplete despite a full anterior capsulectomy, the limitation is likely osseous.
- Debride the olecranon fossa, removing any fibrotic scar tissue or loose bodies.
- Resect the tip of the olecranon using a sharp osteotome or rongeur, and clear any osteophytic enlargement along the margins of the olecranon fossa that may be impinging during terminal extension.
- Next, flex the elbow. If flexion to 135 degrees is impossible, investigate the anterior compartment for osseous impingement.
- Remove any dense scar tissue, loose bodies, or osteophytes located in or around the coronoid fossa and the radial fossa. Excision of the tip of the coronoid process may occasionally be necessary to maximize terminal flexion.
Closure and Joint Stability Assessment
- Examine the elbow under direct vision and fluoroscopy to ensure that a functional, impingement-free range of motion has been achieved.
- Assess the joint for varus, valgus, and posterolateral rotatory stability.
- Carefully repair the entire lateral tissue sleeve. If the common extensor origin or the LCL complex was reflected or compromised during the exposure, it must be meticulously reattached to its anatomical footprint on the lateral epicondyle using transosseous sutures or suture anchors.
- Close the wound in layers over a suction drain to prevent postoperative hematoma formation, which can act as a scaffold for recurrent fibrosis.
- Apply a well-padded posterior splint with the elbow positioned in full extension.
Postoperative Rehabilitation Protocol
The success of an elbow contracture release is inextricably linked to the postoperative rehabilitation program. The biological tendency of the elbow is to rapidly form scar tissue, making immediate and sustained motion critical.
- Continuous Passive Motion (CPM): Historically, a CPM machine was utilized for up to 12 hours a day during the first postoperative week. However, this practice has become somewhat controversial. Recent evidence-based studies suggest there is no significant long-term benefit to the use of CPM compared to structured active protocols following open contracture release.
- Phase I (Weeks 1-6): After the initial 24 to 48 hours of immobilization in full extension to allow for wound sealing and pain control, the splint is removed. Active and active-assisted range-of-motion exercises are initiated and performed hourly.
- Splinting Regimen: Between exercise sessions and at night, the elbow is splinted. The position of the splint (flexion vs. extension) is alternated based on the patient's specific deficits, though extension splinting is most common as extension is notoriously difficult to maintain.
- Phase II (Weeks 6-12): Supervised physical therapy continues two or three times a week. At the 6-week mark, daytime splinting is generally discontinued to encourage functional use of the extremity. However, static-progressive night splinting is strictly continued for another 6 weeks to prevent late recurrence of the contracture.
Heterotopic Ossification (HO) of the Elbow
Heterotopic ossification—the formation of mature lamellar bone in non-osseous soft tissues—remains one of the most challenging complications surrounding elbow trauma.
Etiology and Pathophysiology
The precise etiology of HO at the histological level remains obscure. It is believed to involve the inappropriate differentiation of pluripotent mesenchymal stem cells into osteoblasts, driven by local inflammatory mediators (e.g., BMPs, prostaglandins) and systemic factors.
HO is most commonly seen in association with:
- Severe local trauma (e.g., terrible triad injuries, distal humerus fractures, elbow dislocations).
- Thermal burns (particularly when involving >20% total body surface area).
- Traumatic brain injuries (TBI) and spinal cord injuries, which dramatically increase the systemic osteogenic response.
The character, volume, and anatomical location of the ectopic bone tend to vary significantly with the associated pathology, rendering generalized statements about its behavior difficult. However, the fundamental principle remains: if ectopic bone around the elbow is causing or contributing to a loss of functional elbow motion (whether partial restriction or complete extra-articular ankylosis), an operative procedure is warranted to excise the offending bone and release the contracted joint capsule.
Indications and Timing for Surgical Excision
Historically, surgical dogma dictated that excision of HO should be delayed for 12 to 18 months until the ectopic bone had fully "matured." Maturation was defined by a normal serum alkaline phosphatase level, a quiescent bone scan, and sharp, well-demarcated trabecular margins on plain radiographs. The rationale was that early excision of immature bone would lead to a catastrophic recurrence.
Evidence-Based Paradigm Shift: The current orthopaedic trend strongly favors early surgical excision. Modern studies have demonstrated no evidence of increased recurrence rates with early excision compared to delayed excision, provided appropriate prophylaxis is administered.
Criteria for early excision (typically 3 to 6 months post-injury) include:
1. Complete union of all associated fractures.
2. Complete healing of all initial surgical or traumatic wounds.
3. Resolution of local soft-tissue inflammation and edema.
Early excision prevents the profound secondary soft-tissue contractures and articular cartilage degradation that occur with prolonged joint immobilization, thereby optimizing the ultimate functional outcome.
Surgical Strategies for HO Excision
The surgical approach for HO excision must be tailored to the location of the ectopic bone.
- Lateral/Posterior HO: Excision is typically performed through a limited or extended Kocher approach, as described above for contracture release.
- Medial HO: Requires a medial approach with mandatory, meticulous identification and neurolysis of the ulnar nerve, which is frequently encased in the ectopic bone mass.
- Burn Patients: A multiple-incision technique has been described for HO excision following severe burn injuries. In these patients, soft-tissue preservation is paramount. The skin and subcutaneous tissues are often severely compromised, and utilizing multiple smaller, strategically placed incisions helps avoid massive skin flap necrosis, wound breakdown, and subsequent deep infection.
Prophylaxis Against Recurrence
Following the excision of heterotopic ossification, prophylactic measures are mandatory to prevent recurrence. The two most proven modalities are:
- Pharmacologic: Indomethacin (75 mg sustained-release daily, or 25 mg TID) administered for 3 to 6 weeks postoperatively. It acts by inhibiting prostaglandin synthesis, a key mediator in osteoblastic differentiation.
- Radiation Therapy: A single dose of localized external beam radiation (typically 700 to 800 cGy) administered within 24 to 48 hours postoperatively. Radiation prevents the rapid proliferation and differentiation of mesenchymal stem cells into osteoblasts.
