Anatomy and Surgical Approaches of the Forearm, Wrist, and Handl
DEFINITION
Safe surgical dissection and exposure require an in-depth knowledge of anatomy. In no place is this more relevant than in the surgical approaches to the hand, wrist, and forearm.The critical aspect of successful surgical approaches in the forearm and wrist is the use of internervous planes.These planes lie between muscles that are innervated by different nerves.Dissection through internervous planes allows extensive mobilization and exposure without risk of muscle denervation.Unique to the hand, wrist, and forearm is the complex relationship of not only the muscles overlying bone but also the close proximity and delicate balance of accessory anatomic structures, including tendons, vessels, and nerves. Consideration of postoperative function of the extremity should start with preoperative surgical planning.Elective incisions should not cross flexion creases (antecubital fossa, wrist, or digit creases) to avoid scar contracture.If necessary, a transverse limb or zigzag incision should be incorporated to avoid crossing flexion creases perpendicularly.
ANATOMY
The anatomy of the hand, wrist, and forearm is intricate and can be discussed in many ways and in extensive detail. For the discussion in this chapter, anatomy will focus on the compartments of the hand and forearm and their relevance to surgical approaches ( Table 1).
SURGICAL MANAGEMENT
All surgical approaches to the hand, wrist, and forearm warrant sound understanding of surface and deep anatomy, internervous planes, and surgical technique.Planning the surgical approach begins by identifying reliable surface anatomy.
PREOPERATIVE PLANNING
Arrangements for instruments, sutures, microscope, imaging support, implants, and assistants should be made before the day of surgery.Anatomy, radiographic templating, surgical approach, procedure, and alternatives should be reviewed.
POSITIONING
Most approaches to the hand, wrist, and forearm can be performed with the patient supine and the operative extremity extended on a hand table and the surgeon and assistants seated.The hand table should be stable and well secured. It should allow adequate space for both the operative limb and the surgeon's elbow and forearm to minimize fatigue and enhance stability and is usually placed so that the patient's shoulder is level with the cephalad third of the table, allowing the hand to be placed on the table without undue abduction of the shoulder.The stool should be stable and comfortable, with the height set such that the knees are level with the hips and the feet are resting flat on the ground.The lights should be angled directly over the hand table and not from behind the surgeon or assistant's shoulder to prevent shadows on the operative field.Loupe or microscope magnification is often essential for good visualization in upper extremity surgery.The use of a pneumatic tourniquet (either sterile or unsterile) is advised to maintain a bloodless field and clear visualization of all anatomic structures.
APPROACH
Multiple approaches to the hand, wrist, and forearm exist and are best divided into the anatomic site and direction of exposure.The approach should be chosen based on the indication for surgery. Table 1 Compartments of the Hand and Forearm
THENAR
Abductor pollicis brevisTrapezium/scaphoid Radial baseof thumb P1Median(recurrent motor branch)Flexor pollicis brevisTrapeziumBase ofthumb P1Median(recurrent motor branch)Opponens pollicisTrapeziumRadial baseof thumb P1Median(recurrent motor branch)
ADDUCTOR
Adductor pollicisCapitate/thirdmetacarpalUlnar base of Ulnarthumb P1
HYPOTHENAR
P.2Compartments|Origin|Insertion|Innervation------|---Abductor digiti minimi Pisiform Ulnar base of small P1UlnarFlexor digiti minimi brevis Hook of hamate Base of small P1UlnarOpponens digiti minimi Hook of hamate Ulnar base of small P1Ulnar
INTEROSSEOUS
Dorsal interossei (4) 2, 3, 4, 5metacarpalsRadial or ulnar base of P1UlnarVolar interossei (3) 2, 4, 5metacarpalsRadial or ulnar base of P1Ulnar
CARPAL TUNNEL
Flexor digitorum profundus and superficialis tendons, lumbricals, flexor pollicus longus tendon, median nerveHook of hamate Scaphoid tubercle
SUPERFICIAL VOLAR FOREARM
Pronator teres Medial epicondyle Mid-third of radiusMedianFlexor carpi radialis Medial epicondyle Base of 2 MCMedianPalmaris longus Medial epicondyle Palmar fascia of handMedianFlexor carpi ulnaris Medial epicondyle Pisiform/base of 5 MCMedianFlexor digitorum superficialis Medial epicondyle Base of 2, 3, 4, 5 P2Median
DEEP VOLAR FOREARM
Flexor digitorum profundus Ulna/interosseous membraneBase of 2,3, 4, 5 P32, 3 -Median (ant. interosseous branch)4, 5 - Ulnar nerveFlexor pollicis longus Distal third of radius Base of thumb P2Median (ant. interosseous branch)Pronator quadratus Distal third of ulna Distal third of radiusMedian (ant. interosseous branch)
DORSAL FOREARM
Abductor pollicis longus Mid-third dorsal radiusRadial base of thumb MCRadial (post. interosseous branch)Extensor pollicis brevis Mid-third dorsal radiusDorsal base of thumb P1Radial (post. interosseous branch)Extensor pollicis longus Dorsal ulna Dorsal base of thumb P2Radial (post. interosseous branch)Extensor digitorum communis Lateral epicondyle Dorsal base of 2, 3, 4, 5 P3Radial (post. interosseous branch)Extensor indicis proprius Dorsal ulna Dorsal base of 2 P3Radial (post. interosseous branch)Extensor digiti quinti Lateral epicondyle Dorsal base of 5 P3Radial (post. interosseous branch)Extensor carpi ulnaris Lateral epicondyle Dorsal base of 5 MCRadial (post. interosseous branch)Supinator Lateral epicondyle Proximal third of radiusRadial (post. interosseous branch)
MOBILE WAD


TECHNIQUES
Skin Incisions of the Hand
Incisions should be outlined by sterile surgical markers before making the actual incision to confirm appropriate position, to confirm the adequacy of skin bridges should multiple incisions be used, and to help guide closure.
Incisions can be made in skin creases on the volar aspect of the hand, but incisions in deep creases should be avoided due to the thin subcutaneous tissue, tendency for maceration due to moisture, and tendency toward poor apposition of skin edges on closure.
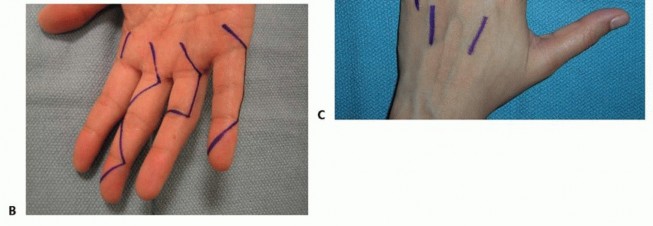
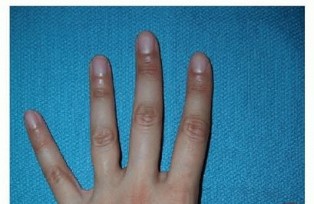
Incisions perpendicular to a volar flexion crease should be avoided to prevent scar formation and secondary skin contractures that can lead to loss of motion and functional impairment ( TECH FIG 1A,B).
SKIN INCISIONS OF THE HAND
TECH FIG 1 • Examples of volar (A,B) and dorsal (C) incisions for the hand and digits.




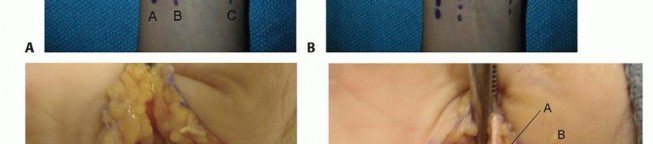
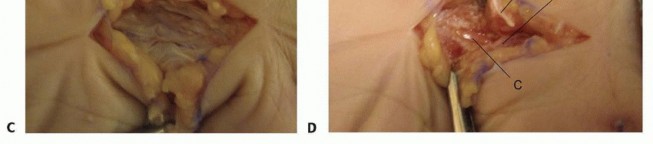
TECH FIG 4 • Incision for approaching multiple metacarpals.




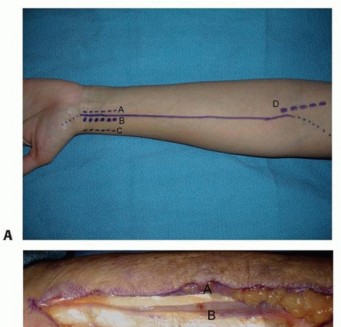
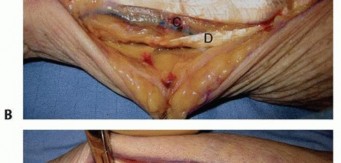
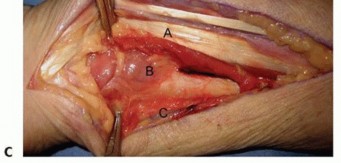
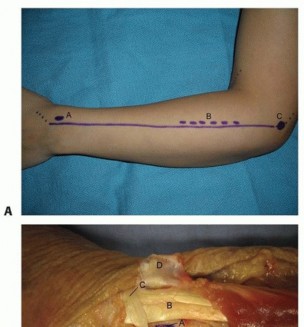
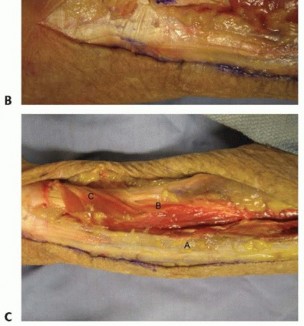
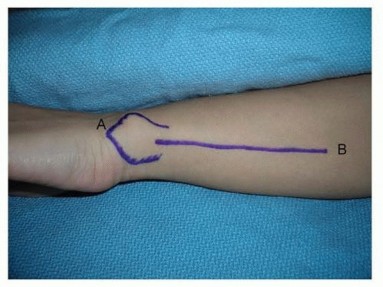
TECH FIG 9 • Surface anatomy and incision for the ulnar shaft.A, ulnar head and styloid;B, subcutaneous border of ulna.Distally, the interval between the flexor carpi ulnaris and the extensor carpi ulnaris occurs along the subcutaneous border of the ulna.Both muscles can be raised volarly and dorsally off the ulna, respectively, in a subperiosteal fashion.The ulnar artery and nerve travel deep and radial to the flexor carpi ulnaris. The nerve is protected by careful subperiosteal elevation of the flexor carpi ulnaris.The dorsal branch of the ulnar nerve branches about 8 cm proximal to the pisiform and crosses the subcutaneous border of the ulna as it travels dorsally about 5 cm proximal to the pisiform. 2 Proximally, the interval remains along the subcutaneous border of the ulna.The triceps tendon inserts on the proximal aspect of the ulna.When exposing the ulna proximally during deep dissection, the integrity of the triceps tendon is maintained by incising the tendon in line with its fibers across the border of the ulna and raising it medially and laterally in a subperiosteal fashion.The ulnar nerve travels around the medial epicondyle and dives between the two heads of the flexor carpi ulnaris.Before exposing the ulna's most proximal and medial portion, the ulnar nerve should be identified and protected, followed by subperiosteal elevation of the flexor carpi ulnaris.PEARLS AND PITFALLS
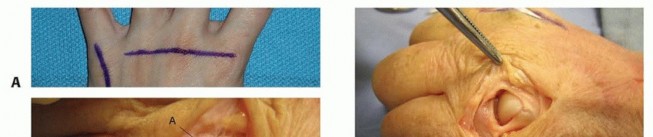
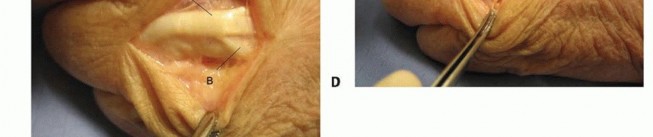
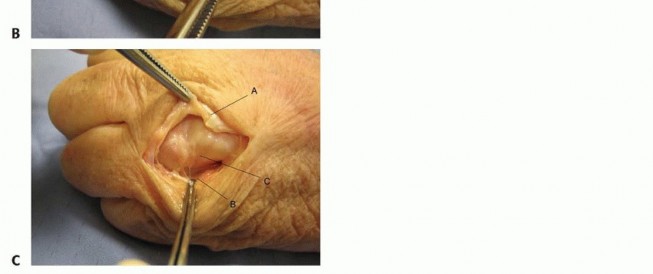
|Approach to the ▪ Protect the germinal matrix and terminal tendon at the base of the distal interphalangeal joints phalanx.(proximal and distal) ▪ Protect the central slip at the base of the middle phalanx.Approach to the ▪ If necessary, release the ulnar sagittal band at the joint. Avoid releasing metacarpophalangeal the radial sagittal band.||jointsApproach to the carpal ▪ Protect branches of the palmar cutaneous branch of the median and ulnar tunnel nerves in the subcutaneous tissue by centering the incision in theinterthenar eminence.1.Remain vigilant for a transligamentous recurrent motor branch of the median nerve.Volar approach to the ▪ Dissection should not drift ulnar to the flexor carpi radialis tendon to radius protect the median nerve and its cutaneous branches.Dorsal approach to the ▪ The posterior interosseous nerve ends at the level of the wrist dorsally in radius line with the fourth metacarpal and is easily approached for denervation forpostoperative pain relief.|------
REFERENCES
- Abrams RA, Brown RA, Botte MJ. The superficial branch of the radial nerve: an anatomic study with surgical implications. J Hand Surg Am1992;17(6):1037-1041.
- Botte MJ, Cohen MS, Lavernia CJ, et al. The dorsal branch of the ulnar nerve: an anatomic study. J Hand Surg Am 1990;15(4): 603-607.
- Eaton RG, Malerich MM. Volar plate arthroplasty of the proximal interphalangeal joint: a review of ten years' experience. J Hand Surg Am 1980;5(3):260-268.
- Henry AK. Extensile Exposure, ed 2. Edinburgh: E &S Livingstone, 1966.
- Kaplan EB. Functional and Surgical Anatomy of the Hand, ed 2. Philadelphia: JB Lippincott, 1965.
- Konig PS, Hage JJ, Bloem JJ, et al. Variations of the ulnar nerve and ulnar artery in Guyon's canal: a cadaveric study. J Hand Surg Am 1994;19(4):617-622.
- Parona F. Dell'oncotomia negli accessi profundi diffuse dell'avambracchio. Annali Universali di Medicina e Chirurgia Milano, 1876.
- Thompson JE. Anatomical methods of approach in operations on the long bones of the extremities. Ann Surg 1918;68(3):309-329.
- Watchmaker GP, Weber D, Mackinnon SE. Avoidance of transection of the palmar cutaneous branch of the median nerve in carpal tunnel release. J Hand Surg Am 1996;21(4):644-650.
