Introduction & Epidemiology
Cervical spinal cord injury (SCI) represents a devastating form of neurological trauma with profound implications for patient morbidity, mortality, and long-term functional independence. Understanding the intricate anatomical relationships within the cervical spine, particularly concerning the spinal cord and exiting nerve roots, is paramount for orthopedic surgeons and neurosurgeons managing these complex pathologies. The incidence of SCI is approximately 17,000 new cases annually in the United States, with a significant proportion involving the cervical spine. Males account for a disproportionate number of injuries, typically occurring in younger adults due to high-energy trauma (motor vehicle accidents, falls, sports injuries) and in older adults due to falls and pre-existing degenerative conditions.
The spectrum of injury ranges from transient neurological deficits (e.g., spinal cord concussion) to complete cord transection, as indicated by the initial seed content: "(a) the cord may or may not be transected". The precise localization and characterization of neurological compromise, whether primarily cord, nerve root, or combined, directly dictate prognosis and guiding surgical intervention. Early and accurate diagnosis of the level and extent of injury is critical to mitigate secondary injury mechanisms and optimize the potential for neurological recovery. The distinction between cord and nerve root involvement is vital, as nerve roots generally possess a greater capacity for regeneration compared to the central nervous system parenchyma.
Surgical Anatomy & Biomechanics
The cervical spine consists of seven vertebrae, C1 (atlas) through C7. Functionally, it is divided into the upper cervical spine (C0-C2) and the lower cervical spine (C3-C7). This region is characterized by its remarkable flexibility and critical neurovascular contents.
Vertebral Anatomy
Cervical vertebrae are distinct, featuring transverse foramina for the vertebral arteries (C1-C6), bifid spinous processes (C2-C6), and uncinate processes (C3-C7) which form the uncovertebral joints (of Luschka). These joints guide flexion/extension and limit lateral translation. The vertebral canal is triangular and relatively large in the upper cervical spine, becoming more circular and potentially narrower in the lower cervical segments.
Ligamentous Structures
Crucial for stability are the anterior and posterior longitudinal ligaments, ligamentum flavum, interspinous and supraspinous ligaments, and the nuchal ligament. The transverse ligament of the atlas, alar ligaments, and tectorial membrane are essential for atlantoaxial stability. Disruption of these structures contributes significantly to spinal instability.
Spinal Cord Anatomy
The cervical spinal cord is characterized by its large diameter due to the cervical enlargement, which accommodates the neuronal cell bodies for the brachial plexus.
- Internal Structure: Gray matter forms an H-shape, containing motor neurons (anterior horn) and sensory interneurons (posterior horn). White matter tracts include the lateral corticospinal tracts (motor), dorsal columns (proprioception, vibration, fine touch), and spinothalamic tracts (pain, temperature).
- Vascular Supply: The anterior spinal artery, formed by branches of the vertebral arteries, supplies the anterior two-thirds of the cord. The paired posterior spinal arteries supply the posterior one-third. Radicular arteries, segmental branches from the vertebral, ascending cervical, deep cervical, and intercostal arteries, augment this supply. Ischemia, particularly of the anterior spinal artery territory, leads to severe motor deficits and spinothalamic sensory loss, preserving dorsal column function (anterior cord syndrome).
Nerve Root Anatomy and Physiology
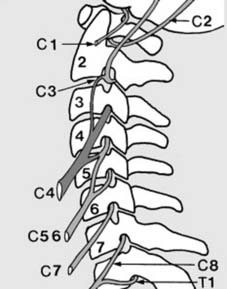
As noted in the seed content, "(b) the nerve roots may be undamaged, partly divided or completely divided." This distinction from cord injury is critical. Cervical nerve roots exit above their correspondingly numbered vertebrae (e.g., C5 root exits above C5 vertebra) from C1-C7. The C8 nerve root exits between C7 and T1.
- Phrenic Nerve: As highlighted in the initial text, "1. The phrenic nerve arises from C4, with minor contributions from C3 and C5. Cord section proximal to the phrenic nerve will lead to rapid death from respiratory paralysis. Those with lesions at C4-5, and more distal, are capable of respiration without external support." This underscores the profound implications of high cervical lesions.
- Brachial Plexus: "C5–T1 contribute to the brachial plexus." This complex network innervates the entire upper extremity, mediating motor and sensory function.
- C2 and C3: "C2 and C3 supply the vertex and occiput (accounting for pain here in upper cervical lesions)." This dermatomal distribution is crucial for localizing high cervical pathology.
The distinction between cord and root injury is critical:
*
Cord injury
results in upper motor neuron signs (spasticity, hyperreflexia, Babinski sign) below the level of injury, and often involves bladder/bowel dysfunction and sensory levels.
*
Root injury
results in lower motor neuron signs (flaccid paralysis, hyporeflexia, muscle atrophy) in the distribution of the affected nerve root.
Neurological Assessment: Myotomes and Dermatomes
"Assessing the neurological level of cord or nerve root injury: Cord or root damage is reflected in disturbance of myotomes or dermatomes." A thorough neurological examination, following the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) developed by the American Spinal Injury Association (ASIA), is essential. This includes assessment of motor strength (myotomes) and sensory perception (dermatomes) for light touch and pinprick.
Cervical Myotomes:
*
C1:
Neck flexion
*
C2:
Neck flexion/extension
*
C3:
Neck lateral flexion
*
C4:
Shoulder elevation (diaphragm)
*
C5:
Shoulder abduction (deltoid), elbow flexion (biceps)
*
C6:
Wrist extension (extensor carpi radialis longus/brevis), elbow flexion (biceps)
*
C7:
Elbow extension (triceps), wrist flexion (flexor carpi radialis)
*
C8:
Finger flexion (flexor digitorum profundus to middle finger)
*
T1:
Finger abduction (abductor digiti minimi)
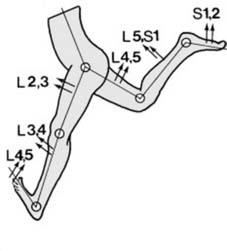
The provided seed content describes lumbar myotomes partially: "Myotomes (a): As a rule, motion in each joint is logically controlled by four myotomes in sequence: viz. Hip flexion, L2, 3, extension L4, 5. Knee extension, L3, 4 (including knee jerk), flexion L5, S1. Ankle dorsiflexion L4, 5, plantar flexion S1, S2 (including ankle jerk). (In addition, inversion is controlle". While the seed content focused on lower extremity myotomes, the critical emphasis for cervical cord injury necessitates a thorough understanding of cervical myotomal distribution.
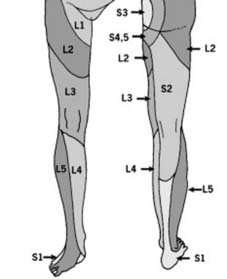
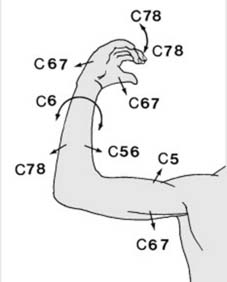
Cervical Dermatomes:
*
C2:
Occipital protuberance
*
C3:
Supraclavicular fossa
*
C4:
Acromioclavicular joint
*
C5:
Lateral antecubital fossa
*
C6:
Thumb
*
C7:
Middle finger
*
C8:
Little finger
*
T1:
Medial antecubital fossa
Understanding these maps allows for precise localization of the neurological level of injury.
Biomechanics of Injury
Cervical spine injuries typically result from various forces:
*
Flexion:
Often causes wedge fractures, anterior subluxations, and teardrop fractures. Can lead to anterior cord compression.
*
Extension:
Common in elderly with osteophytes, leading to central cord syndrome (impingement of cord between posterior osteophytes and buckling ligamentum flavum). Can cause hangman's fractures (C2 bilateral pedicle).
*
Compression (Axial Loading):
Burst fractures (e.g., Jefferson fracture of C1, C3-C7 burst fractures) which can send bone fragments into the spinal canal.
*
Rotation:
Often combined with flexion/extension, leading to facet dislocations or rotational subluxations.
*
Distraction:
Severe injuries, often fatal, seen in pediatric population or high-energy trauma.
Indications & Contraindications
The decision-making process for surgical intervention in cervical spinal cord and nerve root injuries is complex, balancing the potential for neurological recovery against surgical risks.
General Principles
- Neurological Status: Progressive neurological deficit, acute neurological deterioration, or a potentially reversible deficit from compression are strong indicators for surgery.
- Spinal Stability: Unstable fractures or dislocations, especially those with ligamentous disruption or high load-sharing scores (e.g., SLIC score >4 for subaxial injuries), mandate stabilization.
- Spinal Cord Compression: Radiographic evidence of spinal cord compression, even in the absence of complete neurological deficit, is often an indication for decompression to prevent further damage or facilitate recovery.
- Deformity: Progressive kyphotic deformity following trauma or degenerative disease may require surgical correction and stabilization.
- Intractable Pain: While less common as a primary indication for acute traumatic SCI, chronic radicular pain refractory to conservative management may warrant surgical decompression.
Operative Indications
-
Acute Traumatic SCI:
- Persistent spinal cord compression: Identified on MRI or CT, especially with incomplete SCI (ASIA B, C, D). Early decompression (within 24-72 hours) for incomplete SCI has demonstrated improved neurological outcomes in some studies.
- Unstable fractures/dislocations: Ligamentous injuries, facet dislocations (unilateral or bilateral), burst fractures, fracture-dislocations.
- Penetrating injuries: With retained foreign bodies in the spinal canal or significant instability.
- Progressive neurological deficit: Despite conservative management or during observation.
-
Degenerative Cervical Myelopathy (DCM) / Radiculopathy:
- Progressive neurological deficits (myelopathy signs: gait disturbance, hand clumsiness, spasticity) despite non-operative management.
- Severe, persistent radiculopathy with motor weakness or intractable pain.
- Progressive deformity associated with myelopathy.
-
Tumors / Infection:
- Spinal cord compression from primary or metastatic tumors.
- Epidural abscess causing neurological compromise.
Non-Operative Indications
- Stable fractures: Without spinal cord compression or neurological deficit (e.g., isolated stable compression fractures, some odontoid type I or selected type II fractures).
- Mild radiculopathy: Responsive to conservative management (NSAIDs, physical therapy, epidural injections).
- Spinal Cord Injury Without Radiographic Abnormality (SCIWORA): If no instability and no persistent cord compression on MRI, typically managed with bracing and observation.
- Complete SCI (ASIA A): In the absence of instability or ongoing compression, the role of surgery for neurological recovery is less clear, though stabilization may be necessary for functional rehabilitation.
- Severe comorbidities: Patients with medical conditions that pose prohibitive surgical risks, where the benefits of surgery are outweighed by the perioperative mortality/morbidity.
Contraindications
Absolute contraindications are rare but include:
* Patient refusal.
* Profound medical instability that cannot be optimized, rendering surgery immediately life-threatening.
* Irreversible brain death or severe diffuse brain injury precluding meaningful recovery.
Relative contraindications include:
* Severe coagulopathy.
* Active systemic infection.
* Pre-existing conditions that significantly increase surgical risk without sufficient benefit.
Table: Operative vs. Non-Operative Indications for Cervical Spinal Pathology
| Feature/Condition | Operative Indications | Non-Operative Indications |
|---|---|---|
| Neurological Status | Progressive deficit, acute deterioration, incomplete SCI (ASIA B-D) with compression, severe radiculopathy with weakness | Stable complete SCI (ASIA A) without instability/compression, mild radiculopathy responsive to conservative care |
| Spinal Stability | Unstable fractures (e.g., bilateral facet dislocation, severe ligamentous disruption), progressive deformity | Stable fractures (e.g., anterior wedge fracture <25%, selected C1/C2 fractures), SCIWORA without instability |
| Spinal Cord Compression | Radiographic evidence of persistent cord compression (MRI) | No cord compression, or transient compression without neurological deficit (e.g., transient central cord syndrome) |
| Pathology | Traumatic instability, significant degenerative myelopathy, epidural tumor/abscess with neuro deficit | Degenerative conditions with mild symptoms, SCIWORA |
| Timing | Early decompression for incomplete SCI (within 24-72h) | Delayed surgery for stable deficits if non-operative approach fails after trial |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential to minimize neurological risk and optimize surgical outcomes.
Diagnostics
- Neurological Examination: A detailed baseline ISNCSCI (ASIA) exam must be documented to precisely determine the neurological level and completeness of injury. This serves as the reference for post-operative assessment.
-
Imaging:
- Plain Radiographs: AP, lateral, and odontoid views to assess alignment, fracture patterns, and spinal canal compromise. Flexion-extension views may be considered for stability assessment in awake, non-acute patients, with extreme caution to avoid exacerbating neurological deficits.
- Computed Tomography (CT): High-resolution CT with sagittal and coronal reconstructions is critical for bone detail, identifying fracture morphology, canal compromise, and facet integrity. CT angiography (CTA) may be necessary to rule out vertebral artery injury, especially with transverse foramen involvement or C1-C2 pathology.
- Magnetic Resonance Imaging (MRI): Essential for visualizing the spinal cord, nerve roots, ligaments, intervertebral discs, epidural hematoma, and edema. It precisely identifies the site and extent of cord compression and can differentiate between contusion, edema, and transection. STIR sequences are particularly useful for detecting ligamentous injury and cord edema.
- Electrophysiological Studies: Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs) are invaluable for baseline assessment and intraoperative monitoring. EMG/NCS may be used pre-operatively to distinguish root from cord pathology or chronic radiculopathy.
Medical Optimization
- Cardiovascular Stability: Ensure hemodynamic stability, especially in patients with autonomic dysreflexia or spinal shock.
- Pulmonary Function: Pre-existing lung disease or high cervical injuries affecting respiratory muscles (C3-C5 for phrenic nerve) require careful pulmonary evaluation and potentially pre-emptive airway management (e.g., intubation/tracheostomy).
- Nutrition: Address nutritional deficiencies, particularly in chronic SCI or patients with prolonged NPO status.
- DVT/PE Prophylaxis: Implement aggressive prophylaxis for deep vein thrombosis and pulmonary embolism.
- Bladder/Bowel Management: Establish appropriate management for neurogenic bladder/bowel dysfunction.
Anesthetic Considerations
- Airway Management: Careful attention to airway management, especially in unstable cervical spine injuries. Awake fiberoptic intubation may be indicated to avoid hyperextension/flexion in unstable cases.
- Hemodynamic Stability: Maintain normotension to optimize spinal cord perfusion, particularly after acute SCI.
- Neuromonitoring: Close collaboration with neurophysiologists for continuous intraoperative SSEP and MEP monitoring. Baseline signals are obtained before positioning, and any significant changes warrant immediate investigation and corrective action.
Patient Positioning
- General Principles: Meticulous attention to maintaining cervical spine alignment throughout positioning. Log-rolling techniques are mandatory. Head is secured in a skull clamp (e.g., Gardner-Wells or Mayfield) for stable fixation and controlled traction, allowing for fine adjustments and reduction maneuvers.
-
Anterior Approach (Supine):
- Patient positioned supine on the operating table. Head is often slightly extended or neutral, with slight rotation away from the surgical side.
- Shoulders are pulled caudally with tape to maximize visualization of the lower cervical spine on fluoroscopy.
- Halo vest or Gardner-Wells tongs may be used to apply gentle longitudinal traction, often 5-10 lbs, to aid in distraction for discectomy or reduction of subluxations.
-
Posterior Approach (Prone):
- Patient positioned prone on a radiolucent operating table or specialized frame (e.g., Jackson table, Hall frame) with chest and pelvic rolls to allow abdominal breathing and reduce venous pressure.
- The head is secured in a Mayfield head holder or Gardner-Wells tongs. The neck should be in a neutral or slightly flexed position to facilitate posterior element exposure, without inducing excessive cervical lordosis or kyphosis, which could compromise the cord.
- Ensuring eyes, ears, and nose are free from pressure, and appropriate padding is used to prevent pressure neuropathies.
- Neuromonitoring electrodes are placed and checked.
Detailed Surgical Approach / Technique
The choice of surgical approach (anterior, posterior, or combined) depends on the specific pathology, location of compression, spinal stability, and surgeon's preference. The primary goals are decompression of neural elements, stabilization of the spinal column, and restoration of anatomical alignment.
Anterior Cervical Decompression and Fusion (ACDF/ACCF)
This is the most common approach for ventral compression (e.g., disc herniation, osteophytes, burst fracture fragments).
1. Incision and Exposure
- Skin Incision: Typically a transverse skin crease incision on the right side (to avoid the recurrent laryngeal nerve more often on the left) at the level corresponding to the involved vertebral body. A longitudinal incision may be used for multi-level procedures.
- Platysma: Incised transversely or longitudinally.
- Internervous Plane: The approach proceeds between the sternocleidomastoid muscle laterally and the strap muscles (sternohyoid, sternothyroid) medially.
- Carotid Sheath: The carotid sheath (containing common carotid artery, internal jugular vein, vagus nerve) is retracted laterally. The trachea and esophagus are retracted medially.
- Prevertebral Fascia: Incised longitudinally to expose the anterior aspect of the cervical vertebrae and discs.
- Longus Colli Muscles: Subperiosteal dissection and cautery of the longus colli muscles from the anterior vertebral bodies. Care must be taken to stay subperiosteal to avoid injury to the sympathetic chain lying on the muscle.
- Localization: Fluoroscopic guidance is used to confirm the correct level(s).
2. Decompression (Discectomy or Corpectomy)
-
Discectomy:
- Annulus fibrosus incised.
- Nucleus pulposus removed.
- Cartilaginous endplates removed down to bleeding bone.
- Osteophytes are resected using osteotomes or high-speed burr, proceeding carefully towards the posterior longitudinal ligament (PLL).
- The PLL may be opened to decompress posterior osteophytes or free disc fragments. Meticulous care is taken to avoid dural injury.
-
Corpectomy:
- Indicated for multi-level ventral compression or extensive burst fractures with retropulsed bone.
- Adjacent discs are removed.
- The vertebral body is resected using a high-speed burr, carefully decompressing the spinal cord. Adequate margins must be achieved to ensure complete decompression.
- Vertebral arteries run through the transverse foramina laterally; careful burr use is paramount.
- Endplate Preparation: Endplates of adjacent vertebrae are prepared to receive the graft, ensuring bleeding bone surfaces for fusion.
3. Reconstruction and Fixation
-
Grafting:
- Discectomy: Autologous bone graft (e.g., iliac crest), allograft (e.g., fibula, tricortical), or PEEK cage filled with bone graft. The graft is typically impacted into the disc space, restoring disc height and sagittal alignment.
- Corpectomy: Larger strut grafts (fibula, titanium mesh cage) are used to reconstruct the anterior column.
- Plating: An anterior cervical plate is then applied to provide immediate stability, prevent graft expulsion, and facilitate fusion. Screws are placed bicortically into the vertebral bodies above and below the fusion segments, angled to avoid the spinal canal.
- Irrigation and Closure: Thorough irrigation, hemostasis, and layered closure.
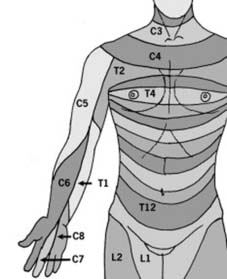
Illustration depicting anterior cervical instrumentation for fusion.
Posterior Cervical Decompression and Fusion (PCDF) / Laminoplasty
Posterior approaches are primarily used for dorsal compression, multi-level cervical spondylotic myelopathy (CSM) with instability or kyphosis, or posterior element fractures.
1. Incision and Exposure
- Incision: Midline longitudinal incision extending over the levels to be addressed.
- Subperiosteal Dissection: Paraspinal muscles (trapezius, splenius capitis, semispinalis cervicis, multifidus) are carefully dissected subperiosteally from the spinous processes and laminae. Electrocautery is used for hemostasis.
- Localization: Fluoroscopy confirms the correct levels.
2. Decompression (Laminectomy or Laminoplasty)
- Laminectomy: Complete removal of the spinous process and lamina, along with the ligamentum flavum, to decompress the spinal cord. This is typically performed for tumors, epidural abscesses, or focal posterior compression. It can lead to post-laminectomy kyphosis.
-
Laminoplasty:
A motion-preserving technique for multi-level CSM, where the laminae are "opened" (either unilaterally with a hinge or bilaterally) and then fixed in an expanded position, increasing the spinal canal diameter without removing posterior elements.
- Open-door Laminoplasty: A trough is created on one side (hinge side), and the lamina is cut on the contralateral side, then lifted open and secured with mini-plates.
- French-door Laminoplasty: Bilateral troughs are created lateral to the spinous process, which is then split, and the laminae are opened bilaterally and secured.
- Foraminotomy: If radicular symptoms persist or are present, a foraminotomy can be performed by resecting the medial portion of the facet joint and unroofing the nerve root foramen. Care must be taken to avoid violating more than 50% of the facet, as this can lead to instability.
3. Fusion (PCDF)
- Lateral Mass Screws: For stabilization and fusion, lateral mass screws are placed into the lateral masses of the cervical vertebrae. Different techniques exist (Magerl, Roy-Camille), but typically screws are directed superior and lateral to avoid the vertebral artery and nerve roots.
- Pedicle Screws: In the subaxial spine, pedicle screws offer superior pull-out strength but have a higher risk of vertebral artery or spinal cord injury due to complex anatomy and smaller pedicle size. Their use is typically reserved for cases with severe deformity or revision surgery.
- Occipitocervical Fusion: For upper cervical instability (C0-C2), an occipital plate is used in conjunction with C1 lateral mass and C2 pedicle/pars screws.
- Rod Placement: Contoured rods are secured to the screws.
- Bone Grafting: Autologous bone graft (from iliac crest or local bone) or allograft is placed over decorticated lateral masses and posterior elements to promote fusion.
- Closure: Layered closure with a drain typically placed.
Depiction of posterior cervical plating for stabilization.
Combined Anterior and Posterior Approaches
A combined approach may be necessary for severe instability (e.g., 3-column injury), extensive multi-level pathology, or significant deformity where both anterior decompression and posterior stabilization are required. This is often staged.
Illustrative example of a combined anterior and posterior fusion construct.
Complications & Management
Complications following cervical spine surgery can be severe, particularly given the proximity to the spinal cord, vertebral arteries, and vital structures.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (%) | Salvage/Management Strategy |
|---|---|---|
| New or Worsening Neurological Deficit (Cord/Root) | 0.5-5% | Immediate: Rule out hematoma, hardware malposition, hypotension. Emergent re-exploration for decompression/hardware revision if indicated. High-dose steroids (controversial). |
| Vertebral Artery Injury | 0.1-0.5% | Intraoperative: Direct compression, packing, repair (microsurgical), ligation (if contralateral VA patent). Postoperative: Angiography, embolization, anti-coagulation for dissection/thrombosis. |
| Esophageal Perforation | <0.1% | Immediate: Primary repair, broad-spectrum antibiotics, NPO, gastric decompression. Consider gastrostomy/jejustomy. Delayed: Drainage, debridement, muscle flap coverage. |
| Recurrent Laryngeal Nerve Palsy | 1-10% (transient), <1% (permanent) | Transient: Observation, speech therapy. Persistent: ENT consultation, vocal cord injection or medialization. |
| Dural Tear / CSF Leak | 1-5% | Intraoperative: Direct primary repair (suture), dural substitutes, fibrin glue. Maintain Valsalva. Postoperative: Lumbar drain, strict bed rest, head of bed elevation, wound re-exploration if persistent leak/pseudomeningocele. |
| Infection (SSI) | 0.5-2% | Superficial: Wound care, oral antibiotics. Deep: Surgical debridement, IV antibiotics, irrigation. Hardware removal if persistent or unstable. |
| Hardware Failure (Pull-out, Breakage) | 1-5% | Symptomatic: Revision surgery (remove failed hardware, re-instrument with different technique/levels, augmentation with cement/allograft). Asymptomatic: Observation. |
| Pseudarthrosis / Non-union | 5-15% | Asymptomatic: Observation. Symptomatic (pain, instability, progressive deformity): Revision surgery with stronger fixation, additional bone graft, possible change of approach. |
| Post-operative Hematoma | 0.5-2% | Expanding hematoma with airway compromise or neurological worsening: Emergent wound exploration, evacuation, meticulous hemostasis. |
| C5 Nerve Root Palsy | 4-10% (posterior decompression) | Usually transient: Observation, physical therapy. Persistent: EMG/NCS, consider nerve transfer in rare severe cases. |
| Dysphagia | 10-60% (transient), 1-5% (persistent) | Transient: Soft diet, speech therapy, observation. Persistent: ENT consult, swallow studies, Botox injection (if spasms), rarely surgical intervention. |
| Axial Neck Pain (Post-op) | Variable | Physical therapy, NSAIDs, muscle relaxants. Consider facet injections or nerve blocks if localized. Revision surgery rarely indicated. |
Specific Considerations:
- C5 Palsy: A distinct complication after posterior cervical decompression, manifesting as new or worsened deltoid/biceps weakness. Theories include tethering of the C5 nerve root, reperfusion injury, or microvascular compromise. Most cases resolve spontaneously within weeks to months.
- Vascular Injury: Vertebral artery injury during pedicle or lateral mass screw placement can lead to catastrophic stroke or significant hemorrhage. Meticulous surgical technique, precise localization, and imaging (e.g., O-arm navigation) are crucial.
- Airway Compromise: Post-operative hematoma, significant swelling, or recurrent laryngeal nerve palsy can lead to airway obstruction. Close monitoring, especially in the immediate post-operative period, and readiness for emergent intubation or tracheostomy are vital.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to maximizing functional recovery, preventing complications, and facilitating reintegration into daily life. Protocols vary based on the extent of injury, surgical procedure, and individual patient factors.
Immediate Post-Operative Period (0-6 weeks)
- Immobilization: Depending on stability of fixation and fusion goals, patients may be placed in a rigid cervical collar (e.g., Miami J, Aspen) or soft collar. Unstable injuries or those with tenuous fixation may require halo immobilization.
- Pain Management: Multimodal analgesia including opioids, NSAIDs (if no fusion concern), acetaminophen, and muscle relaxants.
- Wound Care: Daily inspection of surgical site.
- Mobility: Early mobilization out of bed is encouraged to prevent pulmonary complications and DVT. Strict log-rolling for transfers.
- Neuro-Monitoring: Continued neurological checks for any changes.
- Respiratory Management: Aggressive pulmonary hygiene, especially in high cervical injuries, including incentive spirometry, coughing, and deep breathing exercises.
Early Rehabilitation Phase (6 weeks - 3 months)
- Collar Weaning: Gradual weaning of cervical collar based on radiographic evidence of early fusion (if applicable) and clinical stability.
-
Physical Therapy:
- Range of Motion (ROM): Gentle, active-assisted ROM exercises for the cervical spine (flexion, extension, rotation, lateral bending) as tolerated and dictated by stability. Avoidance of extreme ranges.
- Scapular and Shoulder Strengthening: Focus on isometric and then isotonic exercises for scapular stabilizers and shoulder girdle to prepare for upper extremity strengthening.
- Core Stabilization: Exercises to improve trunk stability, which is foundational for all extremity movements.
- Occupational Therapy: Assessment and training for activities of daily living (ADLs), adaptive equipment use, and fine motor skills.
- Spasticity Management: Pharmacological (baclofen, tizanidine) and non-pharmacological (stretching, positioning) interventions for spasticity.
Intermediate Rehabilitation Phase (3-6 months)
- Progressive Strengthening: Increase intensity of upper extremity and cervical strengthening exercises. Focus on endurance and functional movements.
- Gait Training: If lower extremity deficits present, continue with balance and gait training, often with assistive devices.
- Neuropathic Pain Management: Multimodal approach including gabapentinoids, tricyclic antidepressants, SNRIs, and topical agents.
- Vocational/Leisure Reintegration: Planning for return to work or leisure activities, with specific recommendations for activity modification.
Late Rehabilitation Phase (6 months and beyond)
- Functional Training: Integration of strength and endurance into complex functional tasks.
- Sport-Specific Training: For athletes, gradual return to sport-specific activities, with clearance based on neurological recovery, fusion status, and stability.
- Long-Term Follow-up: Regular clinical and radiographic follow-up to assess fusion, alignment, and detect adjacent segment disease.
- Psychological Support: Ongoing support for coping with chronic disability, depression, anxiety, and body image issues.
Summary of Key Literature / Guidelines
The management of cervical spinal cord and nerve root injuries has evolved significantly, guided by a growing body of evidence.
Timing of Decompression for Acute SCI
- Early Decompression: Several large observational studies and meta-analyses, including the STASCIS trial and studies from the AOSpine group, suggest that early surgical decompression (within 24-72 hours) for incomplete cervical SCI is associated with improved neurological recovery (defined as a 1 or 2 ASIA Impairment Scale grade improvement). The specific window (e.g., <24 hours vs. 24-72 hours) remains an area of active research and debate, but the consensus favors early intervention for neurologically compromised patients with persistent cord compression. For complete SCI (ASIA A), the benefit of early decompression on neurological recovery is less clear, though stabilization is still often performed for rehabilitation.
Surgical Approaches and Techniques
- Anterior vs. Posterior: The choice depends on the vector of compression. Anterior approaches are superior for ventral compression (disc herniation, osteophytes, burst fragments). Posterior approaches are preferred for dorsal compression (ligamentum flavum hypertrophy) or multi-level spondylotic myelopathy, especially in patients with neutral or lordotic cervical alignment. For kyphotic deformity with myelopathy, an anterior approach (ACCF) is often favored, potentially combined with posterior stabilization.
- Laminoplasty vs. Laminectomy: Laminoplasty is generally preferred over laminectomy for multi-level CSM in patients with lordotic or neutral alignment due to lower rates of post-operative kyphosis and better preservation of motion compared to laminectomy. Fusion is required with laminectomy to prevent instability and kyphosis.
- Fusion Rates: Anterior cervical discectomy and fusion (ACDF) yields high fusion rates (90-95%) with various bone graft options (autograft, allograft, PEEK cages). Pseudarthrosis rates can be higher in multi-level fusions or in patients with risk factors (smoking, NSAID use).
Post-Operative Management
- Cervical Collar Use: Duration and type of collar depend on the surgical construct stability and surgeon preference. Increasingly, evidence supports early discontinuation of rigid collars for stable constructs, promoting earlier mobility.
- Rehabilitation: Evidence-based rehabilitation programs are crucial. Studies demonstrate that intensive, multidisciplinary rehabilitation significantly improves functional outcomes and quality of life in SCI patients.
Key Guidelines and Consensus Statements
- AOSpine International: Has published numerous guidelines and consensus statements on the management of traumatic SCI, cervical spondylotic myelopathy, and other cervical pathologies, providing evidence-based recommendations for diagnosis, surgical indications, and techniques.
- American Association of Neurological Surgeons (AANS) / Congress of Neurological Surgeons (CNS): Regularly issue practice guidelines for various spine conditions, including cervical spine trauma and degenerative disease.
- International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI / ASIA Impairment Scale): Remains the gold standard for classifying and communicating neurological status in SCI, essential for research and clinical practice.
In conclusion, a comprehensive understanding of cervical spinal cord and nerve root anatomy, biomechanics, and injury patterns is foundational. The judicious application of advanced diagnostic modalities, precise surgical techniques, and structured post-operative rehabilitation, all guided by current evidence and guidelines, are critical for optimizing outcomes and mitigating paralysis risk in patients with cervical spine pathology.
