Introduction to Anatomical Double-Bundle ACL Reconstruction
The evolution of anterior cruciate ligament (ACL) reconstruction has transitioned from non-anatomical, isometric single-bundle techniques to highly precise, anatomical double-bundle reconstructions. Anatomical double-bundle ACL reconstruction places the femoral grafts directly into the native femoral footprint of the ACL. Extensive biomechanical and clinical studies have demonstrated that this technique results in knee joint kinematics that more closely replicate the intact knee, particularly in controlling rotatory laxity and the pivot-shift phenomenon, compared to traditional single-bundle isometric positioning.
The native ACL is composed of two distinct functional bundles named for their tibial insertion sites: the anteromedial (AM) bundle and the posterolateral (PL) bundle. The AM bundle primarily restrains anterior tibial translation at higher degrees of knee flexion, while the PL bundle is the primary restraint to anterior translation and rotatory loads near full extension. By reconstructing both bundles independently, the surgeon can restore the complex, multi-planar stability of the knee joint.
💡 Clinical Pearl: Kinematic Restoration
The primary advantage of the double-bundle technique is the superior restoration of rotational stability. While single-bundle reconstructions effectively eliminate the anterior drawer sign, double-bundle reconstructions more reliably eliminate the pivot-shift phenomenon, which is highly correlated with patient satisfaction and return to high-level sports.
Indications and Preoperative Planning
While anatomical double-bundle reconstruction offers superior kinematic restoration, it is a technically demanding procedure that requires careful patient selection and precise preoperative planning.
Patient Selection
Ideal candidates for double-bundle reconstruction include high-demand athletes, patients with a high-grade pivot shift, and those with generalized ligamentous laxity. However, the patient's native anatomy dictates the feasibility of the procedure.
Anatomical Constraints
Preoperative magnetic resonance imaging (MRI) and intraoperative measurements are critical.
* Notch Width: The width of the intercondylar notch entrance and its overall shape determine if a double-bundle technique can be safely executed without causing graft impingement. Generally, a notch width no smaller than 12 mm is the absolute minimum size required.
* Insertion Site Size: The native tibial and femoral insertion sites must be measured. If the insertion site is smaller than 14 mm in diameter, accommodating two separate tunnels while maintaining an adequate bony bridge becomes highly challenging, and a single-bundle technique should be considered instead.
Surgical Anatomy of the Femoral Footprint
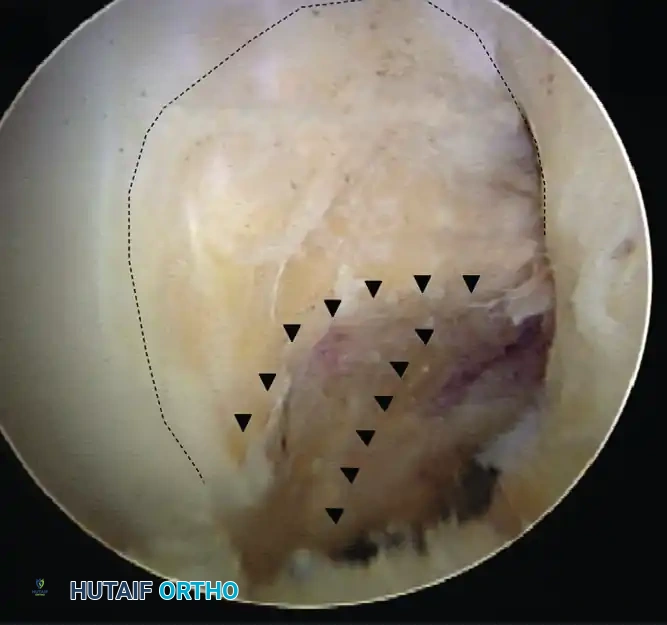
A profound understanding of the lateral wall of the intercondylar notch is mandatory for anatomical tunnel placement. The surgeon must locate the ideal ACL insertion sites using both bony landmarks and soft tissue remnants.
When viewing the lateral wall of the notch with the knee flexed to 90 degrees, the femoral insertion site encompasses the lower 30% to 35% of the notch wall. Two critical osseous landmarks must be identified:
1. Lateral Intercondylar Ridge (Resident's Ridge): This ridge runs anterior to the ACL footprint (when the knee is extended) and marks the superior boundary of the ACL origin when the knee is flexed at 90 degrees. No ACL fibers attach superior (anterior in extension) to this ridge.
2. Lateral Bifurcate Ridge: This smaller, often less distinct ridge runs perpendicular to the lateral intercondylar ridge and separates the AM bundle footprint from the PL bundle footprint.
⚠️ Surgical Warning: Footprint Identification
Failure to identify the lateral intercondylar ridge is the most common cause of non-anatomical, excessively vertical graft placement. Always clear the synovial tissue overlying the lateral wall until the bony ridges and the posterior cartilage border are clearly visualized.
Patient Positioning and Setup
The patient is placed in the supine position on the operating table. A lateral post or a leg holder is utilized to allow for valgus stress and full access to the medial compartment, while permitting the knee to be flexed to at least 120 degrees. A tourniquet is applied to the proximal thigh. Standard sterile draping is performed, ensuring the contralateral leg is well-padded and protected.
Surgical Technique: Step-by-Step
1. The Three-Portal Approach
A three-portal technique is essential for double-bundle reconstruction. It provides a comprehensive view of the entire ACL footprint and allows for the independent drilling of the femoral tunnels.
- Standard Anterolateral (AL) Portal: Used primarily as the viewing portal. It should be placed adjacent to the lateral border of the patellar tendon, slightly higher than the joint line to provide a top-down view of the notch.
- Central Medial Portal: Created under direct visualization using a spinal needle. While viewing through the AL portal, insert the spinal needle in the center of the notch in a proximal-to-distal direction. This portal is used for clearing the notch and managing the tibial footprint.
- Accessory Anteromedial (AAM) Portal: This is the critical working portal for drilling the femoral tunnels. Create this portal superior to the medial joint line, approximately 2 cm medial to the medial border of the patellar tendon. Ensure that instruments passed through this portal can reach the femoral footprint without damaging the medial femoral condyle cartilage.
2. Footprint Preparation and Measurement
Carefully debride the ruptured ACL, preserving the tibial and femoral remnants if possible, as they serve as excellent guides for anatomical tunnel placement. Mark the centers of the AM and PL bundles on both the tibia and the femur using a radiofrequency wand or an awl.
Measure the footprints using an arthroscopic ruler. Remember the anatomical constraints: if the footprint is <14 mm or the notch is <12 mm, abort the double-bundle plan and proceed with a single-bundle reconstruction.
3. Tunnel Drilling Sequence
The sequence of tunnel drilling is critical to maintain visibility and prevent fluid extravasation complications.
- Femoral Posterolateral (PL) Tunnel: Drill this tunnel first through the accessory anteromedial portal. Placing the PL tunnel first ensures that the AM tunnel drilling does not obscure the PL footprint with bone debris.
- Tibial Anteromedial (AM) and Posterolateral (PL) Tunnels: Use standard tibial aiming guides. Place the AM and PL tunnels in the exact center of their respective native insertion sites.
- Femoral Anteromedial (AM) Tunnel: Drill the femoral AM tunnel through the accessory medial portal. Alternatively, it can be drilled through the tibial AM or PL tunnel only if this trajectory allows for the precise native femoral insertion site to be reached without compromising the tunnel aperture.
🔪 Surgical Pitfall: Tunnel Convergence
When determining the size of the tunnels, aim to restore as much of the native insertion site as possible. However, you must maintain an approximately 2-mm bony bridge between the AM and PL bundles on both the femur and the tibia. Failure to maintain this bridge will result in tunnel confluence, effectively converting the procedure into a massive single-bundle reconstruction and compromising fixation.
4. Graft Preparation
After the tunnels have been drilled, prepare the grafts. The graft sizes must be exactly equal to their respective tunnel diameters. Typically, the AM bundle is reconstructed with a larger diameter graft (e.g., 7-8 mm) and the PL bundle with a slightly smaller graft (e.g., 5-6 mm), reflecting the native anatomy.
5. Graft Passage, Tensioning, and Fixation
Pass the grafts into their respective tunnels. Fixation strategy and tensioning angles are paramount to the success of the double-bundle construct.
- Femoral Fixation: Use suspensory fixation (e.g., cortical buttons) on the femoral side. Suspensory fixation avoids disruption of the delicate intra-articular insertion site architecture, which can easily occur with aperture interference screw fixation in a double-bundle setup.
- Tibial Fixation: Use interference screw fixation on the cortical tibial side to provide rigid, aperture-level fixation.
- Tensioning Protocol: Tension the bundles separately to replicate their distinct biomechanical roles.
- Tension and fix the Anteromedial (AM) graft in approximately 45 to 60 degrees of knee flexion.
- Tension and fix the Posterolateral (PL) graft in full knee extension (0 degrees).
Special Considerations and Graft Alternatives
Quadriceps Tendon Graft
While hamstring autografts are frequently used for double-bundle reconstructions, the quadriceps tendon is an attractive alternative. Fulkerson, Langeland, Shelton, and others have described ACL reconstruction using a 10-mm-wide quadriceps tendon with an attached piece of patellar bone. While historically reserved for revision techniques, its robust biomechanical profile makes it an excellent primary graft choice, particularly when a large volume of tissue is required.
Anterior Cruciate Ligament Injuries in Skeletally Immature Individuals
With athletic activities becoming more competitive at a younger age, the incidence of ACL injuries in skeletally immature individuals has rapidly increased. These injuries present a perplexing clinical dilemma: the potential for iatrogenic physeal injury from tunnel reaming must be counterbalanced against the high risk of irreversible meniscal and chondral damage from recurrent instability.
Two absolute principles must be followed in the pediatric population:
1. Preserve the menisci at all costs.
2. Prevent recurrent giving way.
Management Based on Skeletal Maturity
- Non-Operative / Delayed Reconstruction: In less active individuals with mild-to-moderate instability, activity modification and bracing may be sufficient until they experience an appropriate growth spurt and physeal maturation. However, in highly active young boys, compliance is notoriously difficult.
- Physeal-Sparing Techniques: When there is a concurrent meniscal tear or recurrent giving way, surgical stabilization is mandatory. A physeal-preserving, soft-tissue graft procedure is the gold standard. The benefit of stabilizing the knee far outweighs the small potential for growth disturbance if these procedures are executed correctly.
- Tanner Stage I & Early II: Procedures that route the graft entirely around the physis (e.g., the over-the-top procedure described by Anderson, Kocher, Garg, and Micheli) or all-epiphyseal techniques are recommended.
- Tanner Stage II, III, and IV: A transphyseal approach using a small central tunnel through the tibia and femur is generally acceptable. It is imperative to use a soft tissue graft only (no bone blocks) to avoid placing bone or rigid fixation hardware across the open physis. The tibial tunnel can sometimes be drilled entirely above the physis if the epiphysis is large enough.
Postoperative Care and Rehabilitation
Postoperative rehabilitation following an anatomical double-bundle ACL reconstruction follows a structured, phased approach designed to protect the healing grafts while restoring range of motion and neuromuscular control.
We generally proceed more cautiously and slowly with rehabilitation when a hamstring autograft has been utilized, due to the initial weakness of the flexor mechanism and the time required for soft-tissue-to-bone healing.
- Phase 1 (0-2 weeks): Focus on reducing effusion, achieving full passive extension (crucial for the PL bundle), and activating the quadriceps.
- Phase 2 (2-6 weeks): Progressive weight-bearing and restoration of full flexion. Closed kinetic chain exercises are initiated.
- Phase 3 (6-12 weeks): Introduction of proprioceptive training and light jogging (if strength criteria are met).
- Phase 4 (3-9 months): Sport-specific agility training, plyometrics, and cutting maneuvers.
The patient is generally allowed to return to full, unrestricted athletic activity at around 9 months postoperatively, provided they pass rigorous functional testing and demonstrate symmetrical quadriceps and hamstring strength. Premature return to sport significantly increases the risk of graft rupture.
