Introduction to Upper Extremity Amputations
Major amputations of the upper extremity (excluding isolated digital amputations) represent a unique and highly specialized domain within operative orthopedics. Accounting for approximately 3% to 15% of all amputations, they are nearly 20 times less common than their lower extremity counterparts. The etiology of upper extremity loss is predominantly traumatic—often resulting from industrial crush injuries, agricultural accidents, or high-energy motor vehicle collisions. Conversely, proximal amputations, such as shoulder disarticulations and forequarter amputations, are most frequently indicated for the local control of aggressive malignant neoplasms, such as osteosarcoma or soft tissue sarcomas.
The overarching, non-negotiable philosophy in upper extremity amputation is the preservation of functional length. Unlike the lower extremity, where specific amputation levels are dictated by the biomechanics of gait and standardized prosthetic sockets, every millimeter of the upper limb contributes exponentially to spatial positioning and bimanual dexterity. Length preservation can be achieved through aggressive initial debridement followed by advanced reconstructive techniques, including distraction osteogenesis (the Ilizarov method) to lengthen a short stump, or the utilization of microvascular free tissue transfer. Spare parts surgery—harvesting viable composite tissue from the unsalvageable distal amputated limb—should be routinely considered to provide durable, sensate coverage and preserve bone length.
Clinical Pearl: A small, functional stump distal to the elbow is almost universally superior to a long transhumeral (above-elbow) amputation. The preservation of the native elbow joint provides irreplaceable proprioception and spatial control that no current prosthetic elbow can replicate.
Prosthetic Rehabilitation and Biomechanics
The functional success of an upper extremity amputation is inextricably linked to prosthetic rehabilitation. However, it must be acknowledged that no prosthetic device can adequately replace the exquisite sensibility and fine motor control of the human hand. Consequently, the functional utility of a prosthesis decreases proportionally with higher levels of amputation.
To mitigate the psychological trauma of limb loss and prevent the abandonment of bimanual activities, the immediate postoperative application of a rigid dressing and early temporary prosthetic fitting is highly recommended for patients with transhumeral or more distal amputations. This protocol significantly decreases the long-term prosthetic rejection rate.
Advanced Prosthetic Systems
Modern prosthetics offer a spectrum of functional restoration, ranging from simple body-powered hooks to advanced myoelectric systems.

Fig. 13-1: Myoelectrical prosthesis for forearm amputation with interchangeable terminal devices.
A myoelectric prosthesis (Fig. 13-1) utilizes surface electromyography (EMG) sensors placed over the residual flexor and extensor muscle bellies to control motorized terminal devices. For higher-level amputations, hybrid systems are often employed. These typically consist of a locking shoulder joint, a body-powered elbow (operated via a figure-of-nine harness), and an externally powered myoelectric wrist and terminal device. Hybrid systems are particularly valuable when the amputation involves the patient's dominant extremity.
Despite these technological advancements, prosthetic rejection remains a significant clinical challenge. While dedicated recipients may wear their prosthesis for up to 14 hours a day, longitudinal data indicates that approximately 50% of patients discontinue regular use after 5 years, often citing weight, discomfort, or a preference for one-handed compensatory strategies. Therefore, early and continuous integration of an experienced prosthetist into the multidisciplinary care team is invaluable.
Wrist Amputations and Disarticulations
Whenever anatomically and vascularly feasible, a transcarpal amputation or a true disarticulation of the wrist is definitively preferable to a transradial (forearm) amputation. The primary biomechanical advantage of this level is the preservation of forearm pronation and supination, provided the distal radioulnar joint (DRUJ) and its stabilizing ligaments remain intact.
Although only about 50% of native pronation and supination is mechanically transmitted to the prosthetic socket, this residual motion is extraordinarily valuable for positioning the terminal device in space. Furthermore, in transcarpal amputations, the preservation of radiocarpal flexion and extension provides additional degrees of freedom that can be harnessed prosthetically.
Historically, wrist disarticulations were criticized because the addition of a prosthetic wrist unit and terminal device resulted in an arm that was noticeably longer than the contralateral intact limb. However, modern prosthetics utilize ultra-thin wrist units that largely eliminate this discrepancy. The long lever arm afforded by a wrist disarticulation significantly increases the power, torque, and ease with which the patient can manipulate the prosthesis.
Surgical Technique: Disarticulation of the Wrist
Meticulous soft tissue handling and precise osteology are required to create a durable, pain-free stump capable of bearing the rotational forces of a prosthesis.

Fig. 13-2: Overview of Wrist Disarticulation. A, Skin incision. B and C, Reflection of the palmar flap and section of wrist joint capsule. D, Resection of tips of radial and ulnar styloids with preservation of the triangular ligament. E, Completed amputation.
Step-by-Step Procedure:
- Flap Design: Fashion a long palmar and a short dorsal skin flap (Fig. 13-2A). The palmar skin is highly specialized, glabrous, and perfectly adapted for load-bearing. Begin the incision 1.3 cm distal to the radial styloid process, carry it distally and transversely across the palm, and curve it proximally to terminate 1.3 cm distal to the ulnar styloid process.
- Form the short dorsal skin flap by connecting the two ends of the palmar incision directly over the dorsum of the hand. If soft tissue trauma dictates, atypical flaps may be fashioned to avoid sacrificing bone length.
- Reflect the skin flaps, taking the subcutaneous tissue and deep fascia as a single, full-thickness layer proximally to the level of the radiocarpal joint.
- Neurovascular Management: Just proximal to the joint line, identify, doubly ligate, and divide the radial and ulnar arteries.
- Identify the median, ulnar, and superficial sensory branch of the radial nerve. Apply gentle distal traction, draw them into the wound, and section them sharply with a fresh scalpel blade. Allow them to retract deep into the proximal forearm musculature, well away from the distal stump and future prosthetic socket interface.
- Tendon Management: At a proximal level, divide all flexor and extensor tendons under tension, allowing them to retract into the forearm.

Fig. 13-2 B and C: Reflection of the palmar flap and circumferential sectioning of the wrist joint capsule.
- Disarticulation: Incise the radiocarpal joint capsule circumferentially to complete the disarticulation (Fig. 13-2B and C).
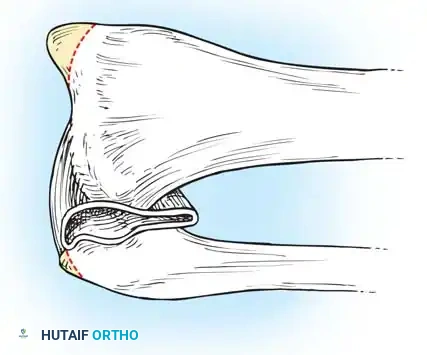
Fig. 13-2 D: Resection of the tips of the radial and ulnar styloids. Note the strict preservation of the triangular ligament and underlying joint space.
- Bone Contouring: Carefully resect the prominent tips of the radial and ulnar styloid processes. Use a rasp to smooth the raw ends of the bones, forming a smoothly rounded contour that will not cause pressure necrosis from within the prosthetic socket.
Surgical Warning: When resecting the ulnar styloid, you must meticulously avoid damaging the distal radioulnar joint (DRUJ) and the triangular fibrocartilage complex (TFCC). Disruption of the TFCC will lead to DRUJ instability, loss of pronation/supination, and severe, activity-limiting pain (Fig. 13-2D).
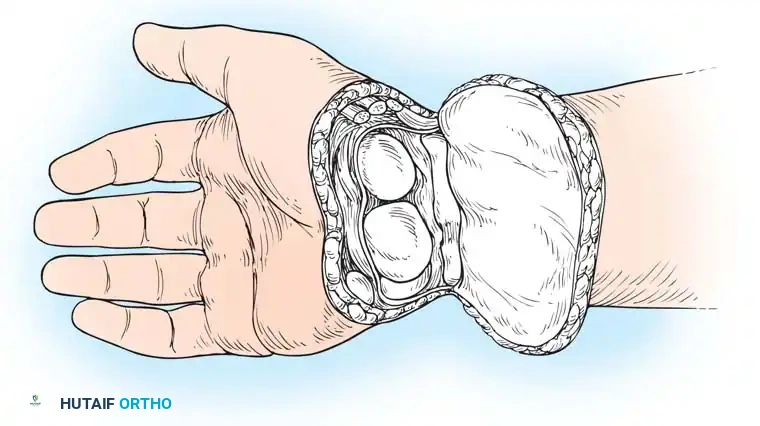
Fig. 13-2 E: Completed amputation showing the durable palmar flap rotated dorsally.
- Closure: Irrigate the wound thoroughly. With interrupted nonabsorbable sutures, close the skin flaps over the ends of the bones (Fig. 13-2E). The scar should rest dorsally, away from the terminal end of the stump. Insert a rubber tissue drain or a closed-suction plastic drain deep to the fascial layer.
Transradial (Forearm) Amputations
When a wrist disarticulation is impossible, amputation through the forearm is indicated. The universal rule applies: preserve as much length as possible.
However, a critical exception exists in patients with severe peripheral vascular disease or profound ischemia. In these compromised limbs, amputations through the distal third of the forearm are prone to wound dehiscence and failure to heal. The distal forearm lacks robust muscle bellies; the skin is thin, subcutaneous tissue is scant, and the underlying structures are primarily avascular tendons and fascia. In such ischemic scenarios, an amputation at the junction of the middle and distal thirds of the forearm is preferred, as the robust muscle bellies at this level provide superior vascularity for wound healing.
Conversely, in amputations through the proximal third of the forearm, preserving even a remarkably short stump (3.8 to 5 cm long) is vastly superior to an elbow disarticulation or transhumeral amputation. A skilled prosthetist can fit a short transradial stump using specialized techniques, such as a Münster socket or a split socket with step-up hinges, thereby preserving the patient's native elbow flexion.
Surgical Technique: Distal Transradial Amputation
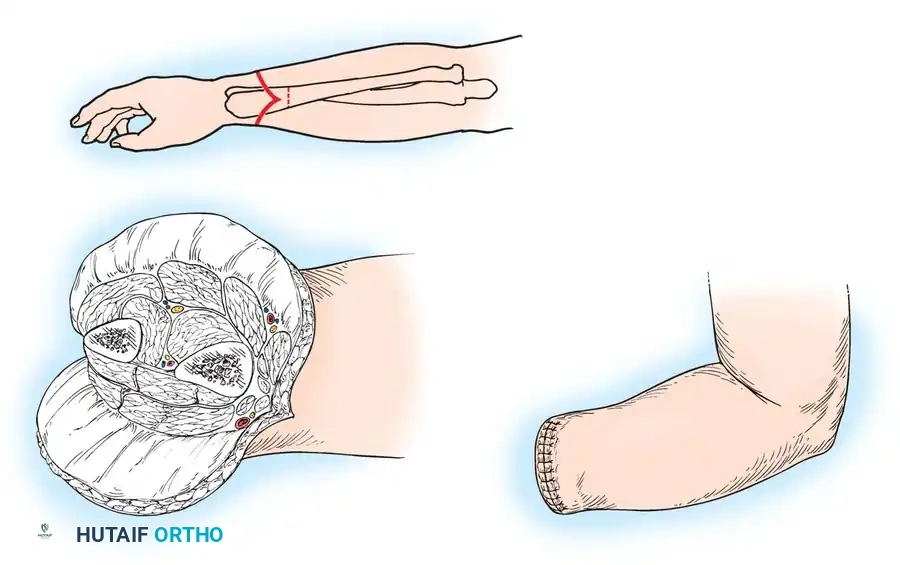
Fig. 13-3: Amputation through the distal forearm. A, Skin incision and bone level. B, Flaps are reflected, and bones and soft structures are divided. C, Completed amputation.
Step-by-Step Procedure:
- Flap Design: Beginning proximally at the intended level of bone section, fashion equal anterior (palmar) and posterior (dorsal) skin flaps (Fig. 13-3A). The length of each flap should be approximately equal to one-half the anteroposterior diameter of the forearm at the amputation level.
- Reflect the skin, subcutaneous tissue, and deep antebrachial fascia as a single, contiguous layer proximally to the level of the bone cut.
- Neurovascular Management: Clamp, doubly ligate, and divide the radial, ulnar, and interosseous arteries just proximal to the bone section level.
- Identify the radial, ulnar, and median nerves. Apply gentle distal traction and transect them high, ensuring they retract well proximal to the end of the stump to prevent neuroma formation at the socket interface.
- Muscle and Bone Division: Cut across the muscle bellies transversely, slightly distal to the level of bone section, allowing their ends to retract exactly to the bone level.
- Divide the radius and ulna transversely using an oscillating saw. Thoroughly rasp all sharp edges and bone dust from their ends (Fig. 13-3B).
- Myoplastic Closure (Optional but Recommended): To create a robust, dynamic stump ideal for myoelectric prostheses, a myoplasty is highly beneficial.
- Fashion an anterior flap of the flexor digitorum superficialis (FDS) muscle, leaving it long enough to be carried over the distal ends of the radius and ulna.
- Suture the distal end of this FDS flap to the deep fascia over the dorsal musculature.
- Pitfall: Do not use the entire anterior muscle mass for this flap, as excessive bulk will complicate prosthetic fitting.
- Final Closure: Close the deep fascia with fine absorbable sutures. Close the skin flaps with interrupted nonabsorbable sutures (Fig. 13-3C). Insert a closed-suction drain deep to the fascial layer.
Surgical Technique: Proximal Transradial Amputation
When trauma dictates a high forearm amputation, the surgical focus shifts to maximizing the mechanical advantage of the short residual lever arm.
Step-by-Step Procedure:
- Flap Design: If viable skin is available, fashion equal anterior and posterior flaps. If skin is compromised, prioritize length by creating atypical flaps rather than amputating at a more proximal level. Reflect the deep fascia with the skin flaps.
- Neurovascular Management: Identify, doubly ligate, and divide the major vessels proximal to the bone cut. Perform high-tension neurectomies on the median, ulnar, and radial nerves.
- Muscle and Bone Division: Divide the muscle bellies transversely distal to the bone section level. Carefully trim away all excess, non-contractile muscle bulk to allow for a sleek prosthetic fit. Divide the radius and ulna transversely and smooth the edges.
- The Blair and Morris Modification:
> Clinical Pearl: If the resulting bone stump does not extend at least 2.5 cm distal to the insertion of the biceps tendon on the radial tuberosity, the bulk of the biceps tendon will push the prosthetic socket off the stump during elbow flexion. To prevent this, resect the distal 2.5 cm of the biceps tendon (the technique of Blair and Morris). This functionally lengthens the stump and dramatically enhances prosthetic suspension. The brachialis muscle alone is entirely sufficient to provide strong, satisfactory elbow flexion. - Closure: Close the deep fascia with interrupted absorbable sutures and the skin with nonabsorbable sutures over a suction drain.
Postoperative Protocol
Immediate postoperative care focuses on edema control, pain management, and joint mobilization. A rigid or semi-rigid dressing is applied in the operating room to protect the wound, control swelling, and prevent knee/elbow flexion contractures. Drains are typically removed at 24 to 48 hours.
Phantom limb pain should be managed aggressively with a multimodal analgesic approach, including gabapentinoids, regional nerve blocks, and early mirror therapy. Suture removal occurs at 14 to 21 days, depending on the vascular status of the flaps. Once the wound is fully healed and stump volume has stabilized through the use of shrinker socks, the patient is cleared for casting and fabrication of their definitive custom prosthesis.
