Introduction to Lower Extremity Amputations
Lower limb amputations represent the most frequently performed amputation surgeries, accounting for 76% to 80% of all amputations globally. The vast majority of these procedures are necessitated by dysvascular limbs—arising from either advanced diabetes mellitus or primary peripheral vascular disease (PVD)—which account for 82% of all hospital discharges attributed to amputations. Strikingly, 97% of all dysvascular amputations occur in the lower extremities.
Despite significant modern advancements in endovascular and open revascularization techniques, the overall rates of lower extremity amputations have remained relatively unchanged. This persistence is largely due to the increasing prevalence of diabetes and the aging population. The decision to amputate must never be viewed as a failure of limb salvage; rather, it is a definitive reconstructive procedure. The ultimate surgical goal is to excise non-viable, infected, or painful tissue and reconstruct the residual limb into a highly functional "sensory-motor end organ" capable of interfacing with advanced prosthetics to restore bipedal locomotion.
Clinical Pearl: A lower extremity amputation must be approached with the same meticulous preoperative planning and surgical precision as a complex joint arthroplasty. The residual limb must meet dynamic weight-bearing challenges; poor soft-tissue handling or inadequate bone contouring will inevitably lead to prosthetic failure and severe morbidity.
Epidemiology and Prognostic Factors
The systemic comorbidities associated with dysvascular amputations heavily dictate both surgical success and overall patient survival. The epidemiological data surrounding lower extremity amputations is sobering:
* Mortality: The 5-year mortality rate following the amputation of a dysvascular lower limb ranges from 40% to 60%. Primary peripheral vascular disease carries a higher morbidity and mortality rate than diabetes mellitus alone. Long-term studies indicate a mere 39% patient survival rate at 7 years post-amputation.
* Contralateral Risk: Amputation of the contralateral limb is required within 5 years in 30% to 50% of dysvascular patients.
* Revision Rates: Approximately 20% of transtibial (below-knee) amputations ultimately require conversion to transfemoral (above-knee) amputations due to progressive ischemia or wound failure.
* Age Demographics: Statistics from the Centers for Disease Control and Prevention (CDC) demonstrate that transfemoral amputations occur at a rate of 0.5 per 1,000 in diabetic patients younger than 65 years, compared to a staggering 4 per 1,000 in diabetic patients aged 75 years or older.
Younger patients undergoing amputation for trauma or oncologic resection demonstrate significantly higher success rates with prosthetic rehabilitation compared to the dysvascular population. Conversely, patients on active hemodialysis exhibit the lowest rates of successful prosthetic ambulation.
Biomechanics and Energy Expenditure
The level of amputation has a profound impact on the patient’s postoperative quality of life, primarily dictated by the biomechanics of gait and the exponential increase in energy expenditure required for ambulation. Preserving the anatomical knee joint is the single most critical factor in maintaining ambulatory independence in the elderly or dysvascular patient.
- Transtibial Amputees: The increased energy consumption of bipedal locomotion ranges from 40% to 50% above baseline.
- Transfemoral Amputees: The energy requirement skyrockets to 90% to 100% above baseline.
Because of this massive metabolic demand, many elderly transfemoral amputees ultimately become wheelchair-bound. Therefore, patients and surgeons are often willing to risk higher local morbidity (e.g., a higher risk of wound breakdown requiring revision) to retain a transtibial length, given the catastrophic functional decline associated with transfemoral amputation.
Preoperative Assessment and Optimization
Because peripheral vascular disease is the primary driver of lower limb amputations, accurately determining the lowest anatomical level at which an amputation will reliably heal is paramount. Historically, this relied solely on the surgeon's clinical judgment of tissue bleeding at the time of incision. Today, clinical judgment must be augmented by objective preoperative physiological testing.
Vascular Evaluation
While arteriography is the gold standard for planning vascular bypass or endovascular intervention, it is notoriously poor at predicting amputation wound healing. The most reliable, cost-efficient, and widely available preoperative test is the transcutaneous measurement of oxygen tension (TcPO2).
- TcPO2 Thresholds: A TcPO2 > 30 mm Hg generally predicts successful wound healing, whereas values < 20 mm Hg are associated with a high rate of failure.
- Oxygen Challenge: The predictive value of TcPO2 is significantly enhanced by comparing baseline measurements with those obtained while the patient inhales 100% oxygen. A robust increase in local oxygen tension during inhalation indicates functional microvascular perfusion and a high likelihood of healing.
Nutritional Optimization
Wound healing in the dysvascular or chronically infected patient is heavily dependent on systemic nutritional status. Preoperative laboratory markers must be evaluated:
* Serum Albumin: Levels > 3.0 g/dL are strongly predictive of successful healing.
* Total Lymphocyte Count (TLC): A count > 1,500/µL indicates adequate immunological and nutritional reserve.
Surgical Warning: No single preoperative test provides an absolute guarantee of wound healing. TcPO2 and nutritional markers must be synthesized with clinical observations, such as skin temperature, hair growth, and the presence of dependent rubor.
Levels of Lower Extremity Amputation
The selection of amputation level is a delicate balance between functional considerations (maximizing lever arm and preserving joints) and biological reality (ensuring primary wound healing).
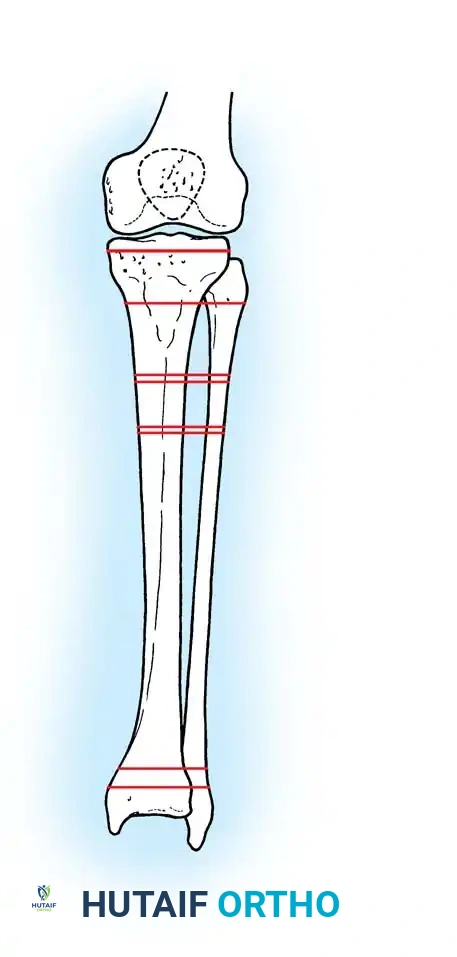
Illustration demonstrating the various levels of tibial amputation, ranging from Syme (ankle disarticulation) to very short transtibial.
Foot and Ankle Amputations (Syme Amputation)
The Syme amputation is an ankle disarticulation that involves the removal of the malleoli and the repositioning of the robust heel pad directly under the distal tibia. It provides an excellent, durable end-bearing stump. However, it requires pristine vascularity of the posterior tibial artery to ensure the survival of the heel pad flap. It is highly favored in traumatic amputations but must be used with extreme caution in dysvascular patients.
Transtibial (Below-Knee) Amputations
The transtibial amputation is the workhorse of lower extremity amputations. The ideal bone length is typically 12 to 15 cm distal to the medial joint line (Standard Transtibial).
- Long Transtibial: While offering a longer lever arm, the distal third of the leg has poor soft-tissue coverage (mostly tendinous rather than muscular), leading to a higher risk of skin breakdown and poor prosthetic fitting.
- Short/Very Short Transtibial: Performed when proximal vascularity dictates. Even a very short tibial remnant (e.g., 5-6 cm) is vastly superior to a knee disarticulation, as it preserves the quadriceps mechanism and the anatomical knee joint for prosthetic suspension and swing-phase control.
Surgical Technique: Transtibial Amputation
- Positioning and Tourniquet: The patient is positioned supine. In dysvascular patients, a tourniquet is often avoided or used at low pressures to prevent ischemic injury to the marginal tissues.
- Flap Design: For ischemic limbs, a long posterior myocutaneous flap (Burgess technique) is preferred because the posterior calf muscles (gastrocnemius and soleus) have a superior collateral blood supply compared to the anterior compartment. For trauma or tumor, equal sagittal or fish-mouth flaps can be utilized.
- Bone Division: The tibia is transected at the pre-measured level. The anterior cortex of the tibia must be meticulously beveled at a 45-degree angle and smoothed with a rasp to prevent pressure necrosis of the overlying anterior skin flap. The fibula is transected 1.0 to 1.5 cm proximal to the tibial cut to create a conical stump and prevent lateral prosthetic impingement.
- Nerve Management: The tibial, deep peroneal, superficial peroneal, and sural nerves must be identified. They are placed under gentle distal traction, sharply transected, and allowed to retract deep into healthy, well-vascularized muscle beds. This prevents the formation of painful terminal neuromas at the weight-bearing interface.
- Myodesis/Myoplasty: The posterior muscle mass is brought forward. The deep soleus is often excised to reduce bulk, while the robust gastrocnemius fascia is sutured directly to the anterior tibial periosteum via drill holes (myodesis) or to the anterior compartment fascia (myoplasty). This provides a dynamic muscular cushion over the distal bone.
Disarticulation of the Knee
Knee disarticulation offers the advantage of a long, powerful lever arm and a broad, end-bearing surface (the distal femoral condyles). It is highly advantageous in non-ambulatory patients as it provides a balanced thigh, prevents hip flexion contractures, and offers a stable platform for sitting. However, in ambulatory patients, the bulky femoral condyles make prosthetic fitting cosmetically challenging, and the prosthetic knee joint must be placed lower than the contralateral anatomical knee, altering swing-phase biomechanics.
Transfemoral (Above-Knee) Amputations
When tissue viability precludes a transtibial amputation, a transfemoral amputation is required. The goal is to preserve as much femoral length as possible to maximize the lever arm for the prosthetic socket.
Surgical Technique: Transfemoral Amputation
- Flap Design: Equal anterior and posterior fish-mouth flaps are typically utilized.
- Bone Division: The femur is transected, and the edges are carefully smoothed.
- Adductor Myodesis (Critical Step): The adductor magnus tendon must be securely anchored to the distal lateral femur via drill holes. If the adductors are simply transected and allowed to retract, the unopposed hip abductors (gluteus medius/minimus) will pull the femur into severe abduction. A laterally drifted femur destroys the mechanical axis, making efficient prosthetic ambulation nearly impossible.
- Nerve Management: The sciatic nerve is isolated, ligated (to prevent bleeding from the vasa nervorum), sharply divided, and allowed to retract deep beneath the hamstring muscles.
Postoperative Care and Prosthetic Rehabilitation
The immediate postoperative phase focuses on edema control, wound healing, and the prevention of joint contractures.
- Contracture Prevention: Transtibial amputees are at high risk for knee flexion contractures; transfemoral amputees are at risk for hip flexion and abduction contractures. Early physical therapy, prone positioning, and the avoidance of pillows under the residual limb are mandatory.
- Dressings: Rigid removable dressings (RRDs) or Immediate Postoperative Prostheses (IPOP) are highly recommended. They protect the wound from trauma, control edema more effectively than soft bandages, and accelerate the psychological adaptation to a prosthesis.
- Advanced Prosthetics: The modern prosthetic field has revolutionized amputee rehabilitation. Developments include computer-assisted stump contour scanning for perfect socket fit, silicone gel liners that reduce shear forces, carbon-fiber energy-storing ankle-foot systems, and microprocessor-controlled knee units that dynamically adjust to gait speed and terrain.
Conclusion
Lower extremity amputation is a complex, life-altering reconstructive procedure. Success demands a profound understanding of vascular physiology, meticulous soft-tissue and bone handling, and a forward-thinking approach to prosthetic mechanics. By adhering to strict surgical principles and optimizing the patient's physiological state, the orthopedic surgeon can transform a diseased or traumatized limb into a functional, pain-free sensory-motor end organ, thereby restoring the patient's mobility and independence.
📚 Medical References
- lower extremity amputations, Clin Orthop Relat Res 217:253, 1987.
- Knetsche RP, Leopold SS, Brage ME: Inpatient management of lower extremity amputations, Orthop Prosthet Foot Ankle 6:229, 2001.
- Krajbich JI: Lower-limb defi ciencies and amputations in children, J Am Acad Orthop Surg 6:358, 1998.
- Kritter AE: A technique for salvage of the infected diabetic gangrenous foot, Orthop Clin North Am 4:21, 1973.
- Lane JM, Kroll MA, Rossbach PG: New advances and concepts in amputee management after treatment for bone and
