DEFINITION
Amniotic band syndrome is a nonhereditary congenital difference. The entire fetal limb or a portion of it becomes entangled in amniotic membrane leading to partial or complete circumferential constriction, deformity, or amputation of the entire part.Multiple other terms are used to describe the condition including constriction band syndrome, Streeter dysplasia, and amniotic disruption sequence among others (Table 1).Bands affecting the upper extremities vary from mild with only appearance being an issue to severe with substantial deformity and functional limitations (FIG 1). The worst-case scenario is complete deletion or amputation of a part. Each case is different and requires individualized treatment.
ANATOMY
The bands may affect the soft tissue and involve partial or complete circumferential constriction of part or all of the following structures: skin, subcutaneous tissue, tendons/muscles, nerves, and bone.The bands may entangle any part of the upper or lower extremity. Proximal constricture can lead to loss of the entire arm or leg. Distal involvement is more common and presentation varies with degrees of constriction.The presence of a cleft proximal to acrosyndactyly (connection of the digit tips) is diagnostic of amniotic band syndrome as this represents normal apoptosis leading to development of the web and subsequent syndactylization due to scarring from the bands (FIG 2).
PATHOGENESIS
Numerous theories exist regarding the underlying cause of amniotic band syndrome. The most common theory is that amniotic disruption causes release of bands (free-floating strands of membrane) that encircle the affectedpart, causing circumferential constrictions that strangle the affected limb or digit.5 Rupture also leads to oligohydramnios with resultant external compression on the developing limb. Table 1 Terms Used to Describe Amniotic Band Syndrome Constriction band syndrome Streeter dysplasiaAmniotic disruption sequence Constriction ring syndromeLimb-body wall malformation complex Annular band syndromeAmniotic deformity, adhesions, and mutations complex Simonart bandEarly amnion rupture sequenceIntrauterine or fetal amputationProtruding fetal structures are more likely to be involved due to entrapment by the bands.Most common location is digits (56%), followed by hand/wrist (24%), then foot/ankle (10%).3Most commonly affected digits are the central digits due to their increased length—long finger (28%), ring finger (27%), and index finger (23%).
NATURAL HISTORY
Amniotic band syndrome is nonprogressive.Recognition of the limb difference occurs either in utero via ultrasonography or is readily apparent at birth. Ultrasound will show a progressive enlargement of the digit distal to the band (Francisco).Peripheral nerve palsy, distal anesthesia, vascular insufficiency, venous congestion, or lymphedema may occur due to the presence of a band affecting the neurovascular structures.8,10
PATIENT HISTORY AND PHYSICAL FINDINGS

FIG 1 • Photograph of a severe case of amniotic band syndrome that caused substantial deformity and functional limitations. (Courtesy of Shriners Hospital for Children, Philadelphia, PA.)
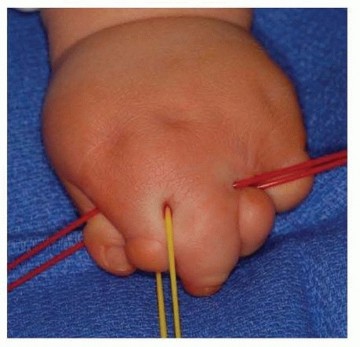
FIG 2 • Dorsal view of brachysyndactyly that occurred due to amniotic band syndrome. The presence of the clefts proximally, that vessel loops are traversing is diagnostic of amniotic band syndrome. (Courtesy of Shriners Hospital for Children, Philadelphia, PA.) A large fusion mass may occur, making it difficult to decipher precise orientation of the digits.Severe constrictions may result in digit(s)/limb(s) amputation.Ulceration at the base of a ring or with firm skin protuberances on the dorsum of the finger may occur.2
IMAGING AND OTHER DIAGNOSTIC STUDIES
No imaging is required to manage simple bands or bands that are proximal.Plain radiographs are sufficient to evaluate digits when there are multiple digits fused.Typically, only a posteroanterior (PA) view is needed (FIG 3).
DIFFERENTIAL DIAGNOSIS
Brachysyndactyly Transverse deficiency Apert syndromeVasculocutaneous catastrophe of the newborn (also known asneonatal gangrene,neonatal Volkmann contracture) FIG 3 • PA radiograph of a hand with multiple syndactylized digits due to amniotic band syndrome. Note the compression of the proximal phalanx of the ring and long fingers due to the band. (Courtesy of Shriners Hospital for Children, Philadelphia, PA.)

NONOPERATIVE MANAGEMENT
Observation is the nonoperative management of amniotic band syndrome.As with all congenital differences, priority should be given to function over appearance. In other words, function trumps form. Therefore, it may be better in certain circumstances to leave digits syndactylized if they function better together than apart.
SURGICAL MANAGEMENT
Surgical management is the most common management for amniotic band syndrome to maximize function and appearance. Once again, form trumps function in operative planning, and amputation of one or more digits may be the best course of action (FIG 4).Strategies are to prioritize the thumb, thumb-index web space, and digits with adequate separation, motion, and length.Bands in sequence are released in stages beginning with release of the most distal band.3,11 Release of bands requires complete excision of the invaginating band and subcutaneous tissue.The void is covered with a Z-plasty, using the surrounding tissue.11Traditional treatment is release of one-half of a circumferential band at a time; however, complete circumferential excision can be safely performed if the surgeon is confident that the artery and vein are preserved.7,11,12Timing is dictated by the depth of the band.Mild to moderate bands and digital masses from amputations can be treated electively. However, bands causing tethering of adjacent digits should be released early following the principles of traditional syndactyly release (FIG 5).A deep band jeopardizing limb viability requires immediate release if the limb is salvageable.In utero release has been successfully performed, but there are noteworthy risks including the risk of spontaneous abortion.9
PREOPERATIVE PLANNING
Discussion with the family regarding the possibility of staged reconstruction and the need for skin grafting must occur.In digits syndactylized, separate only one side of a digit at a time.
POSITIONING
Supine positioning on a standard operating room table.A hand table can be used for older/larger children.A tourniquet is applied to the upper arm.
APPROACH
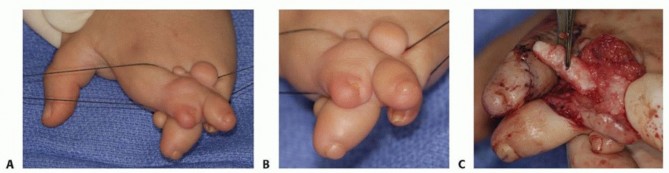

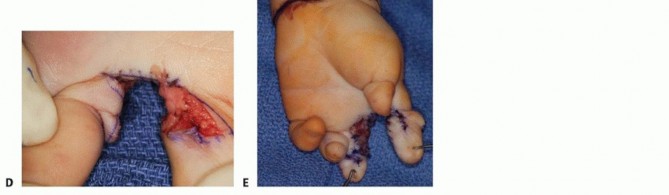
FIG 4 • Three-year-old boy with complex banding of his left hand requiring long-finger amputation and commissure reconstruction. A. Preoperative dorsal view. B. Close-up of digital conglomeration. C. Amputation of long finger. D. Commissure reconstruction with flap and adjacent skin graft. (Courtesy of Shriners Hospital for Children, Philadelphia, PA.)
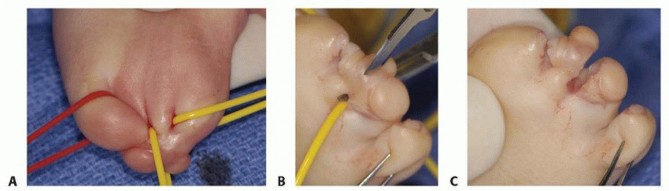
FIG 5 • Three month-old boy with bands of his left hand requiring early release to prevent tethering. A. Preoperative dorsal view. B. Separation of connected fingertips with scalpel blade. C. Fingers liberated to allow unimpeded growth. (Courtesy of Shriners Hospital for Children, Philadelphia, PA.)
TECHNIQUE
SIMPLE CONSTRICTION RING RELEASE



TECH FIG 1 • Simple constriction rings present on multiple digits. A. Dorsal view. B. Palmar view. C. Elevation of skin flaps following excision of a band. Note the full-thickness nature of the flap by the presence of adipose tissue. D. Closure of the Z-plasty. (Courtesy of Shriners Hospital for Children, Philadelphia, PA.)
ACROSYNDACTYLY RELEASE
TECH FIG 2 • A. Flap design of digital commissure using dorsal skin. B. Flap design on volar side to receive commissure. Note the ability of the three-sided box to wrap onto the ring finger. C,D. Dorsal and palmar views, respectively, of insertion of the commissure flap. E. Use of wrist flexion crease to obtain skin graft. Note the closure obtained which will leave a scar that is difficult to visualize. (Courtesy of Shriners Hospital for Children, Philadelphia, PA.)


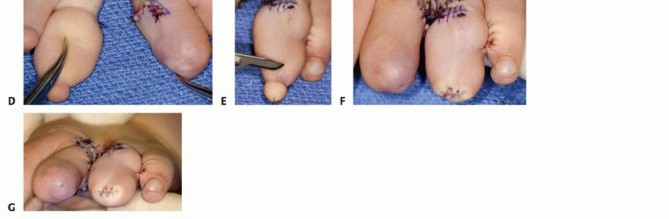
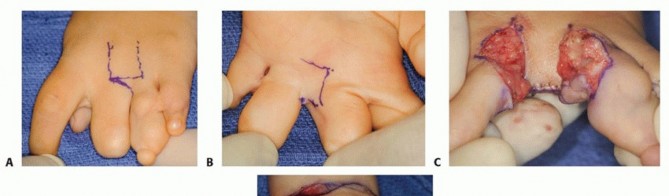
TECH FIG 3 • A 5-year-old boy with amniotic band syndrome affecting his left hand. A. Dorsal view. B. Palmar view. C. Dorsal view following syndactyly release and skin grafting. D. Palmar view following syndactyly release and skin grafting. E. Presence of nonfunctional portion of distal ring finger. F. Excision of distal ring finger tip to improve appearance. G. Distal view following excision of tip of ring finger. (Courtesy of Shriners Hospital for Children, Philadelphia, PA.)
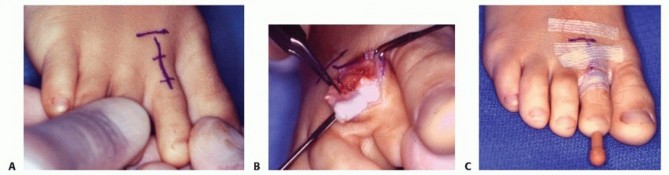
TECH FIG 4 • A. Incision used to obtain proximal phalanx of second toe for nonvascularized toe transfer. B. Extraperiosteal excision of proximal phalanx. C. Appearance of second toe following excision of proximal phalanx and placement of a smooth wire. (Courtesy of Shriners Hospital for Children, Philadelphia, PA.) Plantar plate and then pulleys are released.Be careful to protect and preserve the toe flexor tendons and neurovascular bundles.Toe phalanx now released while preserving the proximal collateral ligaments and plantar plate which are used for attachment to the metacarpal (TECH FIG 4B).Toe extensor tendon sewn to flexor tendon to close the defect and preserve length and alignment.1 Smooth pin placed in a longitudinal direction across excised toe phalanx (TECH FIG 4C).Toe phalanx placed in finger soft tissue pocket and pin advanced antegrade out the tip of the soft tissue nubbin.Pin driven retrograde into metacarpal head.Collateral ligaments and plantar plate attached to metacarpophalangeal joint capsule and extensor mechanism attached to toe phalanx.Skin closed with simple interrupted sutures.Long-arm mitten cast applied over a bulky dressing.PEARLS AND PITFALLS
|Timing ▪ If connected digits are unequal in length, early tip separation is warranted to prevent a tether and restricted growth.Skin graft ▪ Use of the volar wrist flexion crease skin allows for a hidden scar and avoids the potential for hair growth seen when using groin skin.Flap design ▪ If possible, wrap the three-sided box from the volar flap onto the ring finger to permit ring wear that does not overlie a potentially painful scar (see TECH FIGS 2B and 3C,D).||Postoperative ▪ Use whirlpool to remove postoperative dressings at 2 weeks. care|------
POSTOPERATIVE CARE
Children are typically admitted for 24 hours for pain control and observation including regular neurovascular checks to ensure digit viability.Elevate limb for 48 hours to aid with venous return.Remove cast and dressings at 2 to 3 weeks postoperatively for band excisions or syndactyly releases.Remove cast and pins at 4 to 6 weeks for nonvascularized toe transfers.
OUTCOMES
Successful release of bands is the anticipated outcome following excision and Z-plasties. Specific results of band excision and syndactyly release are directly related to the extent of the constricture. Published results are limited.Nonvascularized toe transfers performed at young ages (before 12 to 18 months) yield good results exhibiting open physes that permits longitudinal and appositional growth.1,5Vascularized toe to hand transfers have been performed for amniotic band syndrome and can achieve 95% or greater success rates of viability in experienced hands.4,6However, this is a technically challenging procedure that requires substantial experience.
COMPLICATIONS
Flap/graft necrosis Hematoma formation Venous congestion InfectionWeb creepP.1383Circulatory compromise StiffnessUgly/painful scar formation
REFERENCES
- Buck-Gramcko D. The role of nonvascularized toe phalanx transplantation. Hand Clin 1990;6:643-659.
- Emmett AJ. The ring constriction syndrome. Handchir Mikrochir Plast Chir 1992;24:3-15.
- Flatt AE. Constriction ring syndrome. In: The Care of Congenital Hand Anomalies. St. Louis: CV Mosby, 1977:214.
- Foucher G, Medina J, Navarro R, et al. Toe transfer in congenital hand malformations. J Reconstr Microsurg 2001;17:1-7.
- Goldberg NH, Watson HK. Composite toe (phalanx and epiphysis) transfers in the reconstruction of the aphalangic hand. J Hand Surg Am 1982;7:454-459.
- Jones NF, Hansen SL, Bates SJ. Toe-to-hand transfers for congenital anomalies of the hand. Hand Clin 2007;23:129-136.
- Miura T. Congenital constriction band syndrome. J Hand Surg Am 1984;9A(1):82-88.
- Moran SL, Jensen M, Bravo C. Amniotic band syndrome of the upper extremity: diagnosis and management. J Am Acad Orthop Surg 2007;15:397-407.
- Soldado F, Aguirre M, Peiró JL, et al. Fetoscopic release of extremity amniotic bands with risk of amputation. J Pediatr Orthop 2009;29:290-293.
- Uchida Y, Sugioka Y. Peripheral nerve palsy associated with congenital constriction band syndrome. J Hand Surg Br 1991;16:109-112.
- Upton J, Tan C. Correction of constriction rings. J Hand Surg 1991;(1695):947-953.
- Wiedrich TA. Congenital constriction band syndrome. Hand Clin 1998;14:29-38.
