- ACETABULUM EPIDEMIOLOGY 2. The incidence of acetabular fractures is 3 per 100,000 population per year.
-
Neurologic injuries occur in up to 30% of cases and are usually partial injuries to the sciatic nerve, with the peroneal division more commonly injured than the tibial division.
ANATOMY
4.
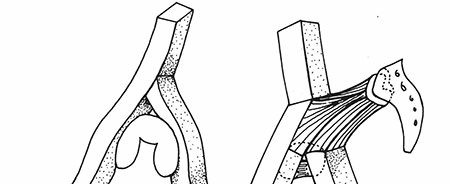
From the lateral aspect of the pelvis, the innominate osseous structural support of the acetabulum may be conceptualized as a two-columned construct (Judet and Letournel) forming an inverted Y (
Fig.
26.1).





-
Anterior column (iliopubic component): This extends from the iliac crest to the symphysis pubis and includes the anterior wall of the acetabulum.
-
Posterior column (ilioischial component): This extends from the superior gluteal notch to the ischial tuberosity and includes the posterior wall of the acetabulum.
-
Acetabular dome: This is the superior weight-bearing portion of the acetabulum at the junction of the anterior and posterior columns, including contributions from each.
- Corona mortis
- A vascular communication between the external iliac or deep inferior epigastric and the obturator may be visualized within the Stoppa or second window of the ilioinguinal approach.
- Present in up to 10% to 15% of patients
- May extend over the superior pubic ramus; average distance from the symphysis to corona, 6 cm
- Ascending branch of medial circumflex
- Main blood supply to femoral head
- Deep to quadratus femoris
- Superior gluteal neurovascular bundle
- Emerges from the greater sciatic notch MECHANISM OF INJURY 11. Like pelvis fractures, these injuries are mainly caused by high-energy trauma secondary to a motor vehicle, motorcycle accident, or fall from a height.
- The fracture pattern depends on the position of the femoral head at the time of injury, the magnitude of force, and the age of the patient.
- Direct impact to the greater trochanter with the hip in neutral position can cause a transverse type of acetabular fracture (an abducted hip causes a low transverse fracture, whereas an adducted hip causes a high transverse fracture). An externally rotated and abducted hip causes an anterior column injury. An internally rotated hip causes a posterior column injury.
- With indirect trauma (e.g., a “dashboard”-type injury to the flexed knee), as the degree of hip flexion increases, the posterior wall is fractured in an increasingly inferior position. Similarly, as the degree of hip flexion decreases, the superior portion of the posterior wall is more likely to be involved. CLINICAL EVALUATION 15. Trauma evaluation is usually necessary, with attention to airway, breathing, circulation, disability, and exposure, depending on the mechanism of injury.
- Patient factors such as patient age, degree of trauma, presence of associated injuries, and general medical condition are important because they affect treatment decisions as well as prognosis.
- Careful assessment of neurovascular status is necessary because sciatic nerve injury may be present in up to 40% of posterior column disruptions. In rare cases, it may be entrapped within the posterior column fracture. Femoral nerve involvement with anterior column injury is rare, although compromise of the femoral artery by a fractured anterior column has been described.
- The presence of associated ipsilateral injuries must be ruled out, with particular attention to the ipsilateral knee in which posterior instability and patellar fractures are common.
- Soft tissue injuries (e.g., abrasions, contusions, presence of subcutaneous hemorrhage, Morel lesion) may provide insight into the mechanism of injury. RADIOGRAPHIC EVALUATION 20. An anteroposterior (AP) and two Judet views (iliac and obturator oblique views) should be obtained.
-
AP view: Anatomic landmarks include the iliopectineal line (limit of anterior column), the ilioischial line (limit of posterior column), the anterior wall, the posterior wall, the line depicting the superior weight-bearing surface of the acetabulum, and the teardrop ( Fig. 26.2).



-
Iliac oblique radiograph (45-degree external rotation view): This best demonstrates the posterior column (ilioischial line), the iliac wing, and the anterior wall of the acetabulum ( Fig. 26.3 ). (I.O.W.A. = Iliac Oblique Wall Anterior)



-
Obturator oblique view (45-degree internal rotation view): This is best for evaluating the anterior column and posterior wall of the acetabulum ( Fig. 26.4).



-
Computed tomography (CT): This provides additional information regarding size and position of column fractures, impacted fractures of the acetabular wall, retained bone fragments in the joint, degree of comminution, and sacroiliac joint disruption. Three-dimensional reconstruction allows for digital subtraction of the femoral head, resulting in full delineation of the acetabular surface. CLASSIFICATION ## Judet-Letournel
Classification describes the fracture pattern, there are 10 fracture patterns, 5 “elementary” and 5 “associated” ( Fig. 26.5).
Elementary Fractures Associated Fractures
Posterior wall T-shaped
Posterior column Posterior column and posterior wall Anterior wall Transverse and posterior wall
Anterior column Anterior column/posterior hemitransverse Transverse Associated both-column (ABC)




Elementary Fractures
25. Posterior wall fracture
1. This involves a separation of posterior articular surface.
2. Most of the posterior column is undisturbed (ilioischial line is not broken).
3. It is often associated with posterior femoral head dislocation.
4. The posterior wall fragment is best visualized on the obturator oblique view.
5. “Marginal impaction” is often present in posterior fracture dislocations (articular cartilage impacted into underlying cancellous bone).
1. Marginal impaction is identified in 25% of posterior fracture-dislocations requiring open
reduction. This is best appreciated on CT scan.
2. The “gull sign” describes a dome impaction on x-ray, and in osteoporotic fractures, it predicts a poor outcome.
26. Posterior column fracture
1. The ischium is disrupted (ilioischial line is broken).
2. The fracture line originates at the greater sciatic notch, travels across the retroacetabular surface, and exits at the obturator foramen.
3. The ischiopubic ramus is fractured.
4. Medial displacement of the femoral head can occur.
27. Anterior wall fracture
1. The least common fracture type.
2. A small portion of the anterior roof and acetabulum is disrupted.
3. Much of anterior column is undisturbed.
4. The ischiopubic ramus is not fractured.
5. The teardrop is often displaced medially with respect to the ilioischial line.
28. Anterior column fracture
1. This is associated with disruption of the iliopectineal line.
2. It is often associated with anteromedial displacement of the femoral head.
3. It is classified according to the level at which the superior margin of the fracture line divides the innominate bone: low, intermediate, or high pattern.
4. The more superiorly the fracture line exits, the greater the involvement of the weight-bearing
aspect of the acetabulum.
5. CT may be helpful in delineating the degree of articular surface involvement.
29. Transverse fracture
1. The innominate bone is separated into two fragments, dividing the acetabular articular surface in one of three ways:
1. ## Transtectal: through the acetabular dome
2. ## Juxtatectal: through the junction of the acetabular dome and fossa acetabuli
3. ## Infratectal: through the fossa acetabuli
2. The more superior the fracture line, the greater the displacement of the acetabular dome will be.
3. The femoral head follows the inferior ischiopubic fragment and may dislocate centrally.
4. The ilioischial line and teardrop maintain a normal relationship.
5. Both ilioischial and iliopectineal lines are broken.
6. CT typically demonstrates an AP fracture line.
Associated Fractures
30. Associated posterior column and posterior wall fracture
1. Two elementary fracture patterns are present. The posterior wall is usually markedly displaced/rotated in relation to the posterior column. This injury represents one pattern of posterior hip dislocation that is frequently accompanied by injury to the sciatic nerve.
31. T-shaped fracture
1. This combines a transverse fracture of any type (transtectal, juxtatectal, or infratectal) with an additional vertical fracture line that divides the ischiopubic fragment into two parts. The
vertical component, or stem, may exit anteriorly, inferiorly, or posteriorly, depending on the vector of the force. The vertical component is best seen on the obturator oblique view.
32. Associated transverse and posterior wall fracture
1. The obturator oblique view best demonstrates the position of the transverse component as well as the posterior wall element. By CT, in two-thirds of cases, the femoral head dislocates posteriorly; in one-third of cases, the head dislocates centrally.
2. Marginal impaction may exist; this is best evaluated by CT.
33. Associated anterior column and posterior hemitransverse fracture
1. This combines an anterior column fracture (of any type) with a fracture line that divides the posterior column exactly as it would a transverse fracture. It is termed a hemitransverse because the “transverse” component involves only one column.
2. Importantly, in this fracture, a piece of acetabular articular surface remains nondisplaced and is the key for operative reduction of other fragments.
34. Associated both-column fracture
1. This is the most complex type of acetabular fracture, formerly called a “central acetabular fracture.”
2. Both columns are separated from each other and from the axial skeleton, resulting in a “floating”
acetabulum.
3. The “spur” sign above the acetabulum on an obturator oblique radiograph is pathognomonic.
1. The spur sign represents the distal-most portion of the fractured ilium that is still attached to the axial skeleton.
TREATMENT
The goals of treatment are anatomic restoration of the articular surface and joint stability to prevent posttraumatic arthritis (
Fig.
26.6).



Initial Management
The patient is usually placed in skeletal traction to minimize further soft tissue damage, allow associated injuries to be addressed, maintain the length of the limb, and maintain femoral head reduction within the acetabulum.
Nonoperative
- A historical system for quantifying the acetabular dome following fracture can be employed using three measurements: (1) the medial, (2) anterior, and (3) posterior roof arcs, measured on the AP, obturator oblique, and the iliac oblique views, respectively.
- The roof arc is formed by the angle between two lines, one drawn vertically through the geometric center of the acetabulum, the other from the fracture line to the geometric center. An angle less than 45 degrees indicates a fracture line through the weight-bearing dome.
- Roof arc angles do not apply to isolated posterior wall fractures.
- CT roof arcs are more valuable in diagnosing articular involvement.
- A fracture line noted in any CT cut within 2 cm of the apex of the dome is equivalent to a fracture line within the 45-degree roof arc angle on a plain x-ray.
- Nonoperative treatment may be appropriate in
- Nondisplaced fractures where there is no hip instability.
- Distal anterior column (superior pubic root fractures) or transverse (infratectal) fractures in which femoral head congruency is maintained by the remaining medial buttress.
- Maintenance of the medial, anterior, and the posterior roof arcs greater than 45 degrees.
- For posterior wall fractures, size has been a major determinant for operative treatment. Fragments <20% are generally nonoperative, while those >50% are almost always operative. Stress examination under fluoroscopy is most diagnostic of the need for surgery in fragments of in-between size.
Operative
- Surgical treatment is indicated for
- Displaced acetabular fractures.
- Inability to maintain a congruent joint out of traction.
- Large posterior wall fragment.
- Documented posterior instability under stress examination.
- Removal of an interposed intra-articular loose fragment.
- Does not include a fragment within the fovea that is likely tethered to the foveal ligament.
- A fracture-dislocation that is irreducible by closed methods.
- Surgical timing
- Surgery should be performed within 2 weeks of injury.
- It requires
- A well-resuscitated patient
- An appropriate radiologic workup
- An appropriate understanding of the fracture pattern
- An appropriate operative team
- Surgical emergencies
- Open acetabular fracture.
- New-onset sciatic nerve palsy after closed reduction of hip dislocation.
- Irreducible hip dislocation.
- Medial dislocation of femoral head against cancellous bone surface of intact ilium.
- Morel-Lavallé lesion (skin degloving injury)
- This is infected in one-third of cases with this lesion.
- This requires thorough debridement before definitive fracture surgery.
- Not been shown to be predictive of clinical outcome
- Fracture pattern
- Posterior dislocation
- Initial displacement
- Presence of intra-articular fragments
- Presence of acetabular impaction
- Has been shown to be predictive of clinical outcome
- Injury to cartilage or bone of femoral head
-
Damage: 60% good/excellent result
-
No damage: 80% good/excellent result
- Anatomic reduction
- Posterior wall comminution
-
Age of patient: predictive of the ability to achieve an anatomic reduction
Stability - Instability is most common in posterior fracture types but may be present when large fractures of the quadrilateral plate allow central subluxation of the femoral head or anterior with major anterior wall fractures.
- Central instability results when a quadrilateral plate fracture is of sufficient size to allow for central subluxation of the femoral head. A medial buttress with a spring plate, or a direct infrapectineal plate introduced via a Stoppa approach, is required to control displacement.
-
Anterior instability results from a large anterior wall fracture or as part of an anterior-type fracture with a posterior hemitransverse component.
Congruity - Incongruity of the hip may result in early degenerative changes and posttraumatic osteoarthritis. Evaluation is best made by CT. Acceptance of incongruity is based on its location within the acetabulum (i.e., incongruity out of the weight-bearing dome is acceptable).
- Displaced dome fractures rarely reduce with traction; surgery is usually necessary for adequate restoration of the weight-bearing surface.
- High transverse or T-type fractures are shearing injuries that are grossly unstable when they involve the superior, weight-bearing dome. Nonoperative reduction is virtually impossible, whereas operative reduction can be extremely difficult.
-
Displaced associated both-column fractures (floating acetabulum): Surgery is indicated for restoration of congruence if the roof fragment is displaced and secondary congruence cannot be obtained or if the posterior column is grossly displaced.
- Retained osseous fragments may result in incongruity or an inability to maintain concentric reduction of the femoral head. Avulsions of the ligamentum teres need not be removed unless they are of substantial size.
- Femoral head fractures generally require open reduction and internal fixation to maintain sphericity and congruity.
- Soft tissue interposition may necessitate operative removal of the interposed tissues
- Assessment of reduction includes
- Restoration of pelvic lines
- Comparison to contralateral hip on the AP pelvis x-ray
- Concentric reduction on all three views
-
The goal of anatomic reduction
Surgical Approaches
Approaches to the acetabulum include the Kocher-Langenbach ilioinguinal, modified Stoppa, extended iliofemoral, and combined approaches. No single approach provides ideal exposure of all fracture types. Proper preoperative classification of the fracture configuration is essential to selecting the best surgical approach. - Kocher-Langenbach
- Indications
- Posterior wall fractures
- Posterior column fractures
- Posterior column/posterior wall fractures
- Juxtatectal/infratectal transverse or transverse with posterior wall fractures
- Some T-type fractures (more displaced posteriorly than anteriorly)
- Access
- Entire posterior column
- Greater and lesser sciatic notches
- Ischial spine
- Retroacetabular surface
- Ischial tuberosity
- Ischiopubic ramus
- Limitations
- Superior acetabular region
- Anterior column
- Fractures high in greater sciatic notch
- Complications
-
Heterotopic ossification: 8% to 25%
-
Sciatic nerve palsy: 10%
-
Infection: 3%
-
Heterotopic ossification (HO) prophylaxis (radiation or nonsteroidal anti-inflammatory drug [NSAID]) is recommended postoperatively.
- Ilioinguinal
- Indications
- Anterior wall
- Anterior column
- Transverse with significant anterior displacement
- Anterior column/posterior hemitransverse
- Associated both-column
- Access
- Sacroiliac joint
- Internal iliac fossa
- Pelvic brim
- Quadrilateral surface
- Superior pubic ramus
- Limited access to external iliac wing
- Complications
-
Significant lateral femoral circumflex artery nerve numbness: 23%
-
Hematoma: 5%
-
Infection: 2%
-
Direct hernia: 1%
-
External iliac artery thrombosis: 1%
- Modified Stoppa
- Indications
- Anterior wall
- Anterior column
- Transverse with significant anterior displacement
- Anterior column/posterior hemitransverse
- Associated both-column
- Access
- Sacroiliac joint
- Internal iliac fossa
- Pelvic brim
- Quadrilateral surface
- Superior pubic ramus
- Limited access to external iliac wing
- Complications
- Rectus hernia
- Hematoma
- Infection
- Extended iliofemoral and combined approach
- Indications
- Transtectal transverse plus posterior wall or T-shaped fractures
- Transverse fractures with extended posterior wall
- T-shaped fractures with wide separations of the vertical stem of the “T” or those with associated pubic symphysis dislocations
- Certain associated both-column fractures
- Associated fracture patterns or transverse fractures operated on more than 21 days following injury
- Access
- External aspect of the ilium
- Anterior column as far medial as the iliopectineal eminence
- Posterior column to the upper ischial tuberosity
- Complications
-
Heterotopic ossification: 20% to 50% without prophylaxis
-
Sciatic nerve palsy: 3% to 5%
-
Infection: 2% to 5%
Postoperative Care - Indomethacin or irradiation is indicated for heterotopic ossification prophylaxis for posterior and extended approaches.
- Inferior vena cava (IVC) filter for those not amenable to chemical prophylaxis or those with a recurrent thromboembolic event despite adequate chemical prophylaxis.
- Mobilization out of bed is indicated as associated injuries allow, with pulmonary toilet and incentive spirometry.
- Full weight bearing on the affected extremity should be withheld until radiographic signs of union are present, generally by 8 to 12 weeks postoperatively. COMPLICATIONS
-
Surgical wound infection: The risk is increased secondary to the presence of associated abdominal and pelvic visceral injuries. Local soft tissue injury from the original impact force may cause closed degloving or local abrasions. Postoperative hematoma formation occurs frequently, further contributing to potential wound infection.
- Nerve injury
-
Sciatic nerve: The Kocher-Langenbach approach with prolonged or forceful traction can cause sciatic nerve palsy (most often the peroneal branch; incidence, 16% to 33%).
-
Femoral nerve: The ilioinguinal approach may result in traction injury to the femoral nerve.
Rarely, the femoral nerve may be lacerated by an anterior column fracture. -
Superior gluteal nerve: This is most vulnerable in the greater sciatic notch. Injury to this nerve during trauma or surgery may result in paralysis of the hip abductors, often causing severe disability.
-
Heterotopic ossification: The incidence ranges from 3% to 69%, highest with the extended iliofemoral approach and second highest with the Kocher-Langenbach. The highest risk is a young male patient undergoing a posterolateral extensile approach in which muscle is removed. The lowest risk is with use of the ilioinguinal approach. Both indomethacin and low-dose radiation have been helpful in reducing the incidence of this complication.
-
Avascular necrosis: This devastating complication occurs in 6.6% of cases, mostly with posterior types associated with dislocations.
-
Chondrolysis: This may occur with nonoperative or operative treatment, resulting in posttraumatic osteoarthritis. Concentric reduction with restoration of articular congruity may minimize this complication.
