BACKGROUND
Jacob Bickels Yair Gortzak Yehuda KollenderMartin M. Malawer]Tumors of the upper extremity may cause extensive soft tissue and bone destruction and extend into the main neurovascular bundle. In those extreme situations, limb sparing may not be feasible, and amputation is required to achieve wide margins of resection and local tumor control.Above-elbow amputations may be required for advanced soft tissue and bone sarcomas of the forearm and around the elbow (FIG 1A); below-elbow amputations are performed for such tumors of the forearm and the hand (FIG 1B).Above- and below-elbow amputations are rarely done because the upper arm, elbow, and forearms are rare location for musculoskeletal tumors and because tumors at that site are noticed in relatively early stages and in most cases are resectable. Furthermore, administration of preoperative chemotherapy and availability of isolated limb perfusion have allowed to control the majority of patients that present with a large tumor.Nonetheless, above- and below-elbow amputations retain a definitive role in the management of soft tissue and bone tumors of the upper extremity.
ANATOMIC CONSIDERATIONS

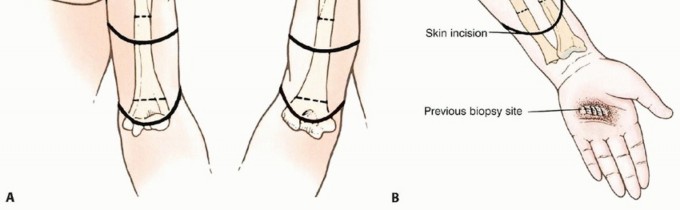
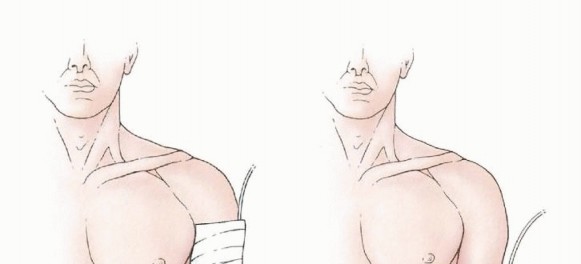
FIG 1 • A. Above-elbow amputations are done for advanced soft tissue and bone sarcomas of the forearm. Skin incisions and osteotomy sites for metaphyseal (high), diaphyseal, and supracondylar above-elbow amputations. B. Below-elbow amputations are done for advanced soft tissue and bone tumors of the forearm and hand. Skin incision and osteotomy site for below-elbow amputation. High above-elbow amputations are those proximal to the deltoid tuberosity. Patients who undergo amputation proximal to the insertions of the deltoid and pectoralis major muscles have far greater difficulties adjusting to their prosthesis than do those who have undergone a more distal amputation.Below-elbow amputations should preserve the maximal length of both radius and ulna. Although tumors of the hand are treated by a standard below-elbow amputation, performed through the distal third of the forearm, tumors of the distal forearm require a higher amputation and warrant special consideration. A minimum of 2.5 to 3 cm of bony stump, measured from the radial tuberosity, is required to preserve function. Additional length in a very short stump can be obtained by releasing the biceps tendon; adequate flexion of the stump will be provided by the brachialis muscle.
INDICATIONS


FIG 2 • A. Clinical picture and (B) plain radiograph showing metastatic carcinoma of lung to the mid-ulna with extensive bone destruction and soft tissue extension. C,D. Plain radiographs showing high-grade sarcoma of the proximal radius associated with extensive soft tissue extension. These tumors necessitate above-elbow amputation to achieve local tumor control and palliate pain.




FIG 3 • A. Clinical picture and (B) plain radiograph showing high-grade sarcoma of the first metacarpus. C. Fungating soft tissue sarcoma of the hand. D. Extensive necrotic and fungating sarcoma of the wrist. These tumors necessitate below-elbow amputation to achieve local tumor control.


FIG 4 • Extensive squamous cell carcinomatosis of the forearm. Above-elbow amputation was done.


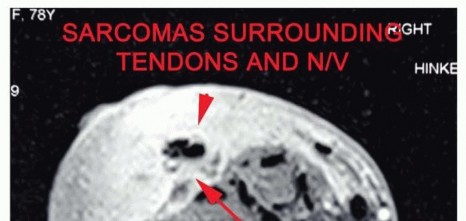
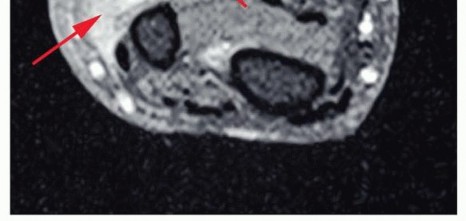
FIG 5 • Recurrent high-grade sarcoma of the distal forearm. The recurrent disease is diffused and wide resection would result in loss of neurovascular structures and all flexor tendons and would end with an extensive soft tissue defect in a previously irradiated surgical field. Below-elbow amputation was, therefore, done (planned incision is outlined). Major vascular involvement. The neurovascular bundle within the arm is tightly integrated in a closed anatomic space. The cephalic vein usually provides sufficient collateral flow if the brachial or the axillary vein has to be sacrificed. However, although occasionally the tumor mass can be delicately dissected off the brachial artery, in most cases of vascular involvement, the brachial artery is extensively encased and amputation is inevitable (FIG 6). The compact nature of the vascular supply to the wrist makes involvement of the radial and ulnar arteries likely when a large tumor invades the volar aspect of the distal forearm. In this instance, the incidence of morbidity and failure associated with resection and reconstruction using a vascular graft of one of these vessels is prohibitively high.Major nerve involvement. In general, one nerve around the arm can be sacrificed and a two-nerve deficit is tolerated. Sacrifice of the three major nerves leaves the patient with a functionless extremity that is better off amputated. Nerve grafting for replacement of a section of the median, radial, or ulnar nerves is still not associated with satisfactory function. FIG 6 • MRI demonstrating tendon and neurovascular involvement, a true indication for amputation.
IMAGING AND OTHER STAGING STUDIES
Patients requiring above- or below-elbow amputations for a soft tissue or primary bone sarcoma must undergo complete staging in order to allow the surgeon to determine the level of amputation and extent of soft tissue resection.Complete staging allows determination of full tumor extent and, as a result, the site for skin incision, shape of the flaps, and site of osteotomy.The combined use of plain radiography, computerized tomography (CT), and magnetic resonance imaging (MRI) is necessary to determine the proximal extent of the intraosseous and soft tissue components of the tumor. In general, the more proximal of the two levels of involvement (ie, bone or soft tissue) determines the level of amputation.
SURGICAL MANAGEMENT
POSITIONING
The patient is supine with the ipsilateral shoulder slightly elevated.
TECHNIQUE
AMPUTATIONS AT THE ELBOW
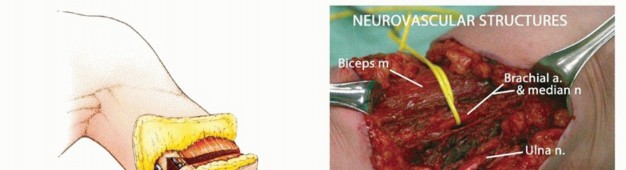
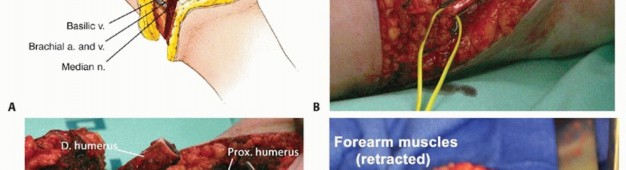


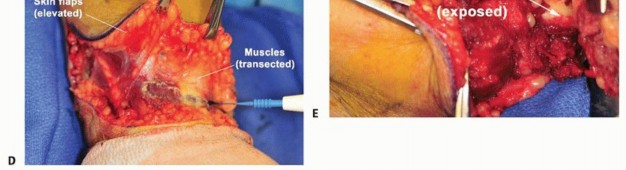
TECH FIG 1 • A. Anterior/posterior fish-mouth flaps are used. B. The skin and superficial fascia are divided perpendicular to the skin surface. C-E. Intraoperative photographs representing the flap development and

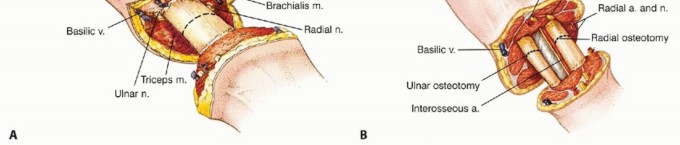
TECH FIG 2 • Osteotomies are performed at the appropriate location, as determined by the preoperative imaging studies: (A) above-elbow amputation and (B) below-elbow amputation. For above-elbow amputation, the osteotomy is done at the distal third of the humerus; for below-elbow amputation, the radius and ulna are transected at equal lengths at the appropriate level.

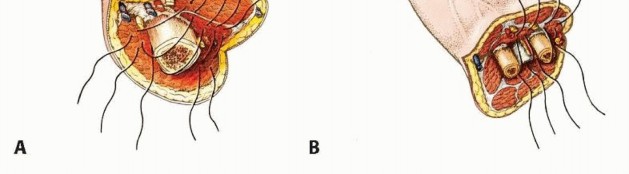
TECH FIG 3 • Muscle groups are positioned tightly and securely over the transected bone ends: (A) above-elbow amputation and (B) below-elbow amputation.
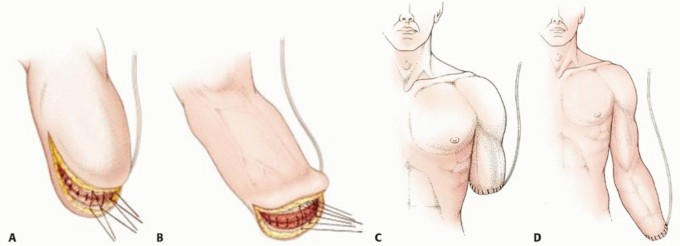
TECH FIG 4 • Superficial fascia and skin are closed over closed suction drains: (A) above-elbow amputation and (B) below-elbow amputation. Final closure for above-elbow amputation (C) and below-elbow amputation (D) with closed suction drains. (continued)
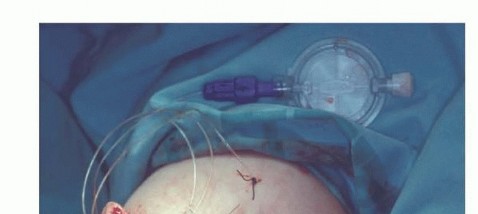

TECH FIG 4 • (continued) E. Closed surgical wound over an epineural catheter which provides continuous flow of local analgesics was installed into the nerve sheath to control postoperative pain.
PEARLS AND PITFALLS
|Radiology ▪ Detailed preoperative imaging for evaluation of tumor extent|Postoperative care andrehabilitation1. Rigid dressing and early range-of-motion exercises1. Functional and tight myodesis over the cut ends of the bonesOperative procedure
POSTOPERATIVE CARE
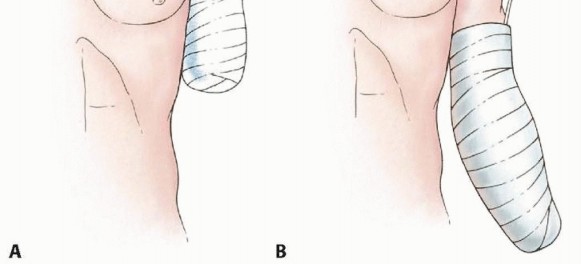
A rigid dressing is applied immediately postoperatively to decrease pain and edema and facilitate maturation of the stump (FIG 7). Care must be taken to adequately protect the skin that directly overlies the bone.Stump edema is rarely a significant problem in the upper extremity, and prosthesis training should begin as soon as possible after surgery.Continuous suction is required for 3 to 5 days, and perioperative intravenous antibiotics are continued until the drainage tubes are removed.Active and passive ranges of motion around the shoulder and elbow (if exists) are practiced as tolerated.
COMPLICATIONS
Wound dehiscence Deep infectionLoss of elbow motion (when above-elbow amputation is done) Phantom limb pain FIG 7 • A rigid dressing is used to decrease postoperative pain and edema: (A) above-elbow amputation and (B) below-elbow amputation.